Links to a list of papers on the trauma-memory argument.
| Note: An edited version will be published in: Uttl, B., Ohta, N, & Siegenthaler, A. L. (Eds.) (2006). Memory and Emotions: Interdisciplinary Perspectives (pp. 259-291). New York: Blackwell. |
Link to Lithuanian translation by Giedrius Sadauskas
 The idea that psychological trauma
can render its victims
amnesic for the traumatic event has been a fixture of
psychotherapy from its
beginnings in the late 19th century. It was firmly
enshrined in
popular culture in the mid-20th century in films like
Random
Harvest (1942), Spellbound (1945), and The
Snakepit (1948).
Despite the rise of biological psychiatry, and a gradual shift
from psychogenic
to somatogenic theories of mental illness, the trauma-memory
argument – and
its companion, recovered-memory therapy – were revived as
post-traumatic
stress disorder was established as the "new hysteria" of our
time –
often with a neuroscientific cover story designed to make it
more appealing to
both professional and nonprofessional consumers of the
contemporary
psychotherapeutic literature.
The idea that psychological trauma
can render its victims
amnesic for the traumatic event has been a fixture of
psychotherapy from its
beginnings in the late 19th century. It was firmly
enshrined in
popular culture in the mid-20th century in films like
Random
Harvest (1942), Spellbound (1945), and The
Snakepit (1948).
Despite the rise of biological psychiatry, and a gradual shift
from psychogenic
to somatogenic theories of mental illness, the trauma-memory
argument – and
its companion, recovered-memory therapy – were revived as
post-traumatic
stress disorder was established as the "new hysteria" of our
time –
often with a neuroscientific cover story designed to make it
more appealing to
both professional and nonprofessional consumers of the
contemporary
psychotherapeutic literature.
The trauma-memory argument proceeds as follows :(Kihlstrom, 1996, 1997, 1998; Shobe & Kihlstrom, 1997)
Traumatic levels of stress sometimes lead victims to invoke mental defenses, such as repression and dissociation, which result in a "psychogenic" or "functional" amnesia for the stressful event itself.
This amnesia affects explicit memory for the trauma, but spares implicit memory, so that representations of the event persist in symptoms such as "body memories".
The presence of such symptoms as "body memories" is a sign that a traumatic event occurred, and that a representation of the traumatic event has been encoded, and is available in memory.
This traumatic memory, ordinarily denied to consciousness, may be recovered, either spontaneously or by means of such techniques as guided imagery, hypnosis, and barbiturate sedation.
In the absence of independent corroboration, the accuracy of the recovered memory may be inferred from its explanatory value in the context of the person’s symptoms – or, simply, from the fact that the person gets better after the memory has been recovered.
Exhumation of the traumatic memory is essential for coping with the trauma itself.
In one form or another, the trauma-memory argument and recovered-memory therapy have been features of clinical lore since the late 19th century, when Pierre Janet and Sigmund Freud announced their respective doctrines of dissociation and repression. In contemporary discourse about trauma, the terms repression and dissociation are sometimes used interchangeably; or, in other cases, the term dissociation seems to be invoked in order to escape the taint of Freudian psychoanalysis.
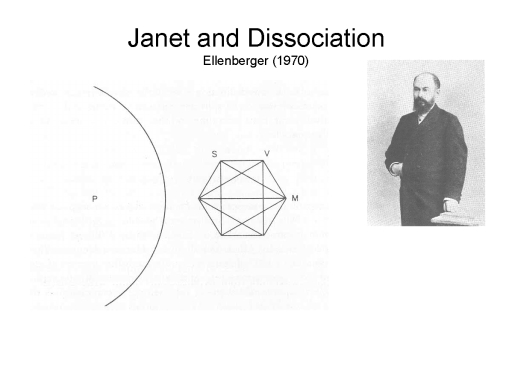 Historically, of course, the doctrine of
dissociation came first
(Ellenberger, 1970; Kihlstrom, Tataryn, & Hoyt, 1993).
Pierre Janet, trained
as both a neurologist and a psychologist, described the
elementary structures of
the mind as psychological automatisms, each representing
a complex act,
finely tuned to the situation (both external and intrapsychic),
preceded by an
idea, and accompanied by an emotion (Janet, 1889). Under normal
circumstances, a
person’s entire repertoire of psychological automatisms is bound
together into
a single unified stream of consciousness. However, under certain
circumstances
one or more of these automatisms can be split off from the rest,
and function
outside either phenomenal awareness, voluntary control, or both.
In Janet’s
case of Irene, for example, ideas related to the death of her
mother – the
sight of her face, the sound of her voice, and the movements of
carrying her
body -- were broken off from the rest of the stream of
consciousness. Janet’s
term for this situation was désagrégation, translated
into English as dissociation.
One circumstance promoting dissociation was psychological
stress, and the
dissociations associated with stress were held to be responsible
for the major
symptoms of hysteria, one of two major categories of neurosis in
Janet’s
system (Janet, 1907). Another circumstance was hypnosis, leading
to the
historical association of hypnosis with hysteria (Kihlstrom,
1979; Kihlstrom
& McGlynn, 1991).
Historically, of course, the doctrine of
dissociation came first
(Ellenberger, 1970; Kihlstrom, Tataryn, & Hoyt, 1993).
Pierre Janet, trained
as both a neurologist and a psychologist, described the
elementary structures of
the mind as psychological automatisms, each representing
a complex act,
finely tuned to the situation (both external and intrapsychic),
preceded by an
idea, and accompanied by an emotion (Janet, 1889). Under normal
circumstances, a
person’s entire repertoire of psychological automatisms is bound
together into
a single unified stream of consciousness. However, under certain
circumstances
one or more of these automatisms can be split off from the rest,
and function
outside either phenomenal awareness, voluntary control, or both.
In Janet’s
case of Irene, for example, ideas related to the death of her
mother – the
sight of her face, the sound of her voice, and the movements of
carrying her
body -- were broken off from the rest of the stream of
consciousness. Janet’s
term for this situation was désagrégation, translated
into English as dissociation.
One circumstance promoting dissociation was psychological
stress, and the
dissociations associated with stress were held to be responsible
for the major
symptoms of hysteria, one of two major categories of neurosis in
Janet’s
system (Janet, 1907). Another circumstance was hypnosis, leading
to the
historical association of hypnosis with hysteria (Kihlstrom,
1979; Kihlstrom
& McGlynn, 1991).
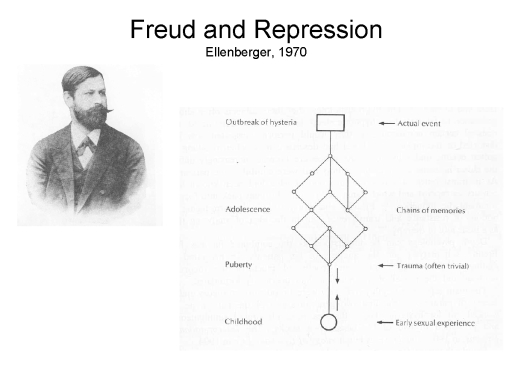 Enter Sigmund Freud. As is well known,
Freud, who also trained
as a neurologist, spent a kind of postdoctoral year (1885-1886)
with Charcot at
the Salpetriere clinic in Paris, where he was introduced to the
wonders of
hysteria and hypnosis, and also began a kind of professional
rivalry with Janet.
Freud actually made his early reputation with the study of
aphasia (Freud,
1891/1953) – and he coined the term agnosia. But he took
his newly acquired
interest in hysteria back to Vienna, and within a couple of
years began to
develop an alternative account of the syndrome in terms of
repression (verdrängt)(Breuer
& Freud, 1893-1895/1953; Freud, 1915/1957) – a concept which
Freud had
borrowed from Herbart’s analysis of unconscious percepts
(Herbart, 1816/1881).
For Freud, early sexual experiences, that were repressed,
combined later with events at the time
of puberty to generate symptoms that appear in adulthood.
Although Freud’s
theory of hysteria shifted from a focus on actual sexual trauma
to sexual
fantasies, repression remained at the heart of the story
(Macmillan, 1997). By
1914, Freud had identified repression as "the foundation-stone
on which the
whole structure of psychoanalysis rests (Freud, 1914/1957, p.
16).
Enter Sigmund Freud. As is well known,
Freud, who also trained
as a neurologist, spent a kind of postdoctoral year (1885-1886)
with Charcot at
the Salpetriere clinic in Paris, where he was introduced to the
wonders of
hysteria and hypnosis, and also began a kind of professional
rivalry with Janet.
Freud actually made his early reputation with the study of
aphasia (Freud,
1891/1953) – and he coined the term agnosia. But he took
his newly acquired
interest in hysteria back to Vienna, and within a couple of
years began to
develop an alternative account of the syndrome in terms of
repression (verdrängt)(Breuer
& Freud, 1893-1895/1953; Freud, 1915/1957) – a concept which
Freud had
borrowed from Herbart’s analysis of unconscious percepts
(Herbart, 1816/1881).
For Freud, early sexual experiences, that were repressed,
combined later with events at the time
of puberty to generate symptoms that appear in adulthood.
Although Freud’s
theory of hysteria shifted from a focus on actual sexual trauma
to sexual
fantasies, repression remained at the heart of the story
(Macmillan, 1997). By
1914, Freud had identified repression as "the foundation-stone
on which the
whole structure of psychoanalysis rests (Freud, 1914/1957, p.
16).  By means of repression, and its supplementary defenses, people
deny themselves
conscious awareness of primitive sexual and aggressive impulses
that conflict
with the demands of reality and the strictures of society --
"monsters from
the Id", in the lovely phrase of Forbidden Planet
(1956), my
favorite science-fiction movie of all time.
By means of repression, and its supplementary defenses, people
deny themselves
conscious awareness of primitive sexual and aggressive impulses
that conflict
with the demands of reality and the strictures of society --
"monsters from
the Id", in the lovely phrase of Forbidden Planet
(1956), my
favorite science-fiction movie of all time.
 Within just a few years, the
psychoanalytic juggernaut had swept
Janet and dissociation into the dustbin of history. Janet’s
views were more
recently revived by the late Ernest R. Hilgard, who proposed a
"neo-dissociation" theory of multiple controls in human thought
and
action, to describe hypnosis and related phenomena (Hilgard,
1977; see also
Kihlstrom, 1992a). Publication of Sybil (Schreiber,
1973) had already
renewed popular interest in multiple personality disorder, which
had been rather
dormant since The Three Faces of Eve (Thigpen &
Cleckley, 1957)(film,
1957) won an Academy Award for Joanne Woodward (in a classic
case of "What
goes around, comes around" Woodward later played a psychiatrist
to Sally Field in
the film version of Sybil, 1976). There followed a
virtual epidemic of
multiple personality disorder in the 1980s and 1990s (Boor,
1982) – including
an amusing contest, of sorts, between Eve and Sybil to determine
who had the
most personalities. Slide 8. In 1980, the third edition
of the Diagnostic
and Statistical Manual of Mental Disorders (DSM-III)
reclassified
psychogenic amnesia, psychogenic fugue, and multiple personality
disorder (MPD)
as "dissociative" disorders (for reviews, see Kihlstrom, 1994;
Kihlstrom, 2001, 2004a; Kihlstrom et al., 1993). In 1984 the
International
Society for the Study of Multiple Personality and Dissociation
held its first
annual conference, and the first scholarly monographs on MPD
appeared in 1986
(Bliss, 1986; Ross, 1986).
Within just a few years, the
psychoanalytic juggernaut had swept
Janet and dissociation into the dustbin of history. Janet’s
views were more
recently revived by the late Ernest R. Hilgard, who proposed a
"neo-dissociation" theory of multiple controls in human thought
and
action, to describe hypnosis and related phenomena (Hilgard,
1977; see also
Kihlstrom, 1992a). Publication of Sybil (Schreiber,
1973) had already
renewed popular interest in multiple personality disorder, which
had been rather
dormant since The Three Faces of Eve (Thigpen &
Cleckley, 1957)(film,
1957) won an Academy Award for Joanne Woodward (in a classic
case of "What
goes around, comes around" Woodward later played a psychiatrist
to Sally Field in
the film version of Sybil, 1976). There followed a
virtual epidemic of
multiple personality disorder in the 1980s and 1990s (Boor,
1982) – including
an amusing contest, of sorts, between Eve and Sybil to determine
who had the
most personalities. Slide 8. In 1980, the third edition
of the Diagnostic
and Statistical Manual of Mental Disorders (DSM-III)
reclassified
psychogenic amnesia, psychogenic fugue, and multiple personality
disorder (MPD)
as "dissociative" disorders (for reviews, see Kihlstrom, 1994;
Kihlstrom, 2001, 2004a; Kihlstrom et al., 1993). In 1984 the
International
Society for the Study of Multiple Personality and Dissociation
held its first
annual conference, and the first scholarly monographs on MPD
appeared in 1986
(Bliss, 1986; Ross, 1986).
With a growing awareness of the problems of returning Vietnam War veterans, as well as the victims of sexual assault, DSM-III also saw the emergence of a new diagnostic category of post-traumatic stress disorder (PTSD). PTSD quickly became a popular diagnosis, as clinicians began noticing its characteristic symptoms – especially anxiety and depression – even in patients who did not appear to have been exposed to the usual sorts of traumas. Increasing societal interest in very real problems of incest and childhood sexual abuse, including the beginnings of the sexual-abuse scandal in the Roman Catholic Church, ignited a revival of Freud’s early theory that hysteria was caused by repressed memories of infantile seduction (Masson, 1984). In 1981, a clinical study of father-daughter incest had made no mention of repression, dissociation, or amnesia (Herman, 1981); in 1987, the same author published a study in which more than 25% of patients in a therapy group for incest survivors were amnesic for their incest (see also Harvey & Herman, 1994; Herman & Schatzow, 1987).
The idea that trauma could be repressed, and that lifting the repression was critical to full recovery, spread like wildfire through American culture. Popular books like The Courage to Heal (Bass & Davis, 1988), probably the best-selling self-help book of all time, fanned the flames:
If you are unable to remember any specific instances... but still have a feeling that something abusive happened to you, it probably did (p. 21).
Many survivors suppress all memories of what happened to them as children.... Coming to believe that the abuse really happened, and that it really hurt you, is a vital part of the healing process (p. 58)....
If you don’t remember your abuse, you are not alone. Many women don’t have memories, and some never get any memories. This doesn’t mean they weren’t abused (p. 81).
 Bass and Davis also published a list of 74
different symptoms
ostensibly associated with sexual abuse, so that readers could
determine for
themselves whether, in fact, they might ever have been abused. A
similar list
even appeared in a professional book published by the American
Psychological
Association (Walker, 1994).
Bass and Davis also published a list of 74
different symptoms
ostensibly associated with sexual abuse, so that readers could
determine for
themselves whether, in fact, they might ever have been abused. A
similar list
even appeared in a professional book published by the American
Psychological
Association (Walker, 1994).
And so, after 100 years, we came full circle: Janet and Freud were vindicated, PTSD was the new neurosis, or at least the new hysteria, and dissociation was the new repression. While the traditional diagnosis of PTSD referred to intrusive memories, the boundaries of the disorder were expanded to include amnesia as well. And because trauma caused dissociation, the dissociative disorders could be reconstrued as forms of PTSD. In 2000, the journal Dissociation was renamed The Journal of Trauma and Dissociation, as if the two were closely related. And in the run up to the publication of DSM-V, there is serious move afoot to reclassify the dissociative disorders as forms of PTSD.
The trauma-memory argument is still with us. As recently as 2004, a highly regarded science writer published a book detailing how unconscious traumatic memories exert toxic effects on mind and body, and how secret traumas can be unlocked and overcome by "power therapies" such as Eye Movement Desensitization and Reprocessing, Thought Field Therapy, and the like (Scarf, 2004). As this paper was being written, Paul Shanley, a former Catholic priest, was convicted in Boston of a single count of child sexual abuse based on an uncorroborated recovered memories from 20 years before. And the New York Times (02/24/05) carried a story about Martha Beck, a sociologist and psychotherapist who writes a self-help column for Oprah Winfrey’s O magazine, who has written a memoir detailing recovered memories of sexual abuse allegedly perpetrated by her father, Hugh Nibley, a prominent Mormon scholar – claims strongly disputed by Beck’s seven siblings (he died at age 94 the day the article was published).
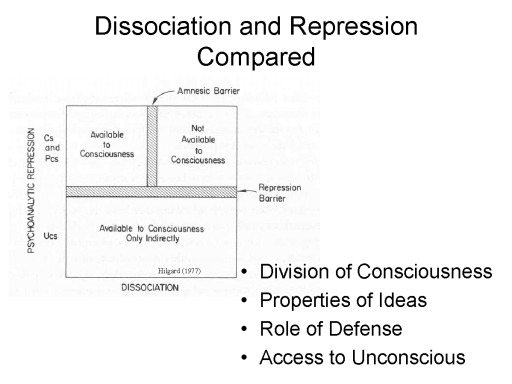 In the contemporary literature, the
terms repression and
dissociation tend to be used interchangeably to refer to
a lack of
conscious awareness of trauma and conflict (Singer, 1990). In
fact, Janet
believed that repression was merely a special form of
dissociation. But Freud
held that dissociation was utterly trivial, and repression was a
separate
process with its own ontological status. In fact, the two
concepts do seem to be
different. As Hilgard (Hilgard, 1977) noted dissociation entails
a vertical
division of consciousness, while in repression the division is
horizontal. For
Freud, available memories are located in the System Cs
and the System Pcs,
while repressed memories are buried in the System Ucs
beneath a barrier
of repression. For Janet, dissociations occur among memories
that are normally
available to consciousness. For Freud, repressed memories have
special emotional
and motivational properties, being closely bound either to
trauma (in his early
theorizing) or with primitive sexual and aggressive impulses (in
his later
work). For Janet, any kind of memory at all can be subject to
dissociation.
In the contemporary literature, the
terms repression and
dissociation tend to be used interchangeably to refer to
a lack of
conscious awareness of trauma and conflict (Singer, 1990). In
fact, Janet
believed that repression was merely a special form of
dissociation. But Freud
held that dissociation was utterly trivial, and repression was a
separate
process with its own ontological status. In fact, the two
concepts do seem to be
different. As Hilgard (Hilgard, 1977) noted dissociation entails
a vertical
division of consciousness, while in repression the division is
horizontal. For
Freud, available memories are located in the System Cs
and the System Pcs,
while repressed memories are buried in the System Ucs
beneath a barrier
of repression. For Janet, dissociations occur among memories
that are normally
available to consciousness. For Freud, repressed memories have
special emotional
and motivational properties, being closely bound either to
trauma (in his early
theorizing) or with primitive sexual and aggressive impulses (in
his later
work). For Janet, any kind of memory at all can be subject to
dissociation.
For Freud, repression is motivated by considerations of defense – the whole point of repression is to prevent us from becoming aware of threats and impulses that would cause us great anxiety. But in Janet’s theory, dissociation just happens as a result of some weakness, or excessive strain, in the stream of consciousness – much the way a chain, when stretched too tightly, will break at its weakest link. Further, Janet appears to believe that one could gain access to dissociated ideas directly, by techniques such as hypnosis that bridge the dissociative gap. By contrast, Freud seems to argue that repressed mental contents can be known only indirectly, by inference: hence Freud’s abandonment of hypnosis and subsequent emphasis on the interpretation of dreams, and of symptoms as symbolic expressions of underlying conflict. In this respect, at least, modern recovered-memory therapy – while certainly inspired by Freud’s ideas about repression – is closer to Janet’s ideas about dissociation.
One point on which both theories agree is that unconscious memories of trauma manifest themselves, unconsciously, in the form of symptoms, dreams, and the like. For Janet, these are the stigmata of hysteria (Janet, 1907). For Freud, "Hysterics suffer mainly from reminiscences." (Breuer & Freud, 1893-1895/1953, p. 7), and their symptoms are evidence of "the return of the repressed" (Freud, 1896, p. 169). Blume (Blume, 1990, p. 93) echoed Freud directly when she wrote that
"hysterical symptoms... represent unremembered trauma or unacknowledged feelings. Because there is a physical distraction, the survivor is at once protected and blocked.... Her body remembers, but her mind does not.
Similarly, van der Kolk (van der Kolk, 1994, p. 253) asserted that unconscious memories of trauma are expressed as somatic symptoms. In his phrase, "the body keeps the score".
Frederickson offered a catalog of the various ways in which repressed memories can return to haunt us (Frederickson, 1992):
Imagistic memory -- incomplete, or exaggerated pictures of the abuse scene;
Feeling memory -- inexplicable emotions pertaining to the event;
Acting-out memory -- including both verbal and bodily acts, as well as actions that occur in dreams.
In terms of modern memory research, we would discuss repression and dissociation in terms of memories of traumatic events that have been encoded, and remain available in storage, but are inaccessible to retrieval. Evidently, the failure of access covers only explicit expressions of traumatic memory; implicit memories of trauma continue to influence the victim’s ongoing experience, thought, and action – in the absence of conscious awareness, and independent of conscious control. Van der Kolk specifically invoked the concept of implicit memory when discussing the aftermath of trauma and abuse:
Research into the nature of traumatic memories indicates that trauma interferes with declarative memory (i.e., conscious recall of experience) but does not inhibit implicit, or nondeclarative, memory, the memory system that controls conditioned emotional responses, skills and habits, and sensorimotor sensations related to experience (van der Kolk, 1994, p. 258).
The explicit-implicit distinction began to emerge in the mid-1980s (Schacter, 1987). Like Hilgard’s neodissociation theory of divided consciousness (Hilgard, 1977), this work inadvertently gave intellectual aid and comfort to the recovered memory movement: At last, science had proved that unconscious memories can exist. But there’s a big difference between inferring the existence of unconscious memories in the laboratory and doing so in the clinic. In the laboratory, implicit memories are commonly expressed as priming effects -- in which, for example, prior study of the word ashcan leads subjects, and even amnesic patients, to complete the word-stem ash- with the word ashcan rather than the far more common ashtray. When subjects who have studied ashcan respond with ashcan more often then subjects who have not, we can plausibly say that the stem-completion is an implicit expression of memory for the prior study episode. This is because we can tie the subject’s task performance to some event in his or her past. But clinicians typically lack the means to independently corroborate what happened to their patients – to confirm the inference that their patients’ behaviors are, in fact, implicit memories of past experiences. Without this independent corroboration, the inference that some symptom actually reflects a repressed traumatic memory is just an opinion. To insist on the correctness of the inference, in the absence of any positive evidence, verges on solipsism.
Let me give you an example from the literature on psychogenic fugue (Lyon, 1985). The patient, known as Jane Doe, could not identify herself or give any helpful information about her identity. During an informal test of her ability to recognize and use common objects, the psychologist Lionel Lyon noticed that she dialed the same telephone number repeatedly. When he called the number himself, the person who answered proved to be the patient’s mother. Now Lyon’s clinical insight was brilliant, but it might have been wrong. Lyon tested his hypothesis, and found that he was right. But suppose that the person on the other end of the line had said that she did not know the patient: Lyon would have had no justification for saying "Yes, you do so too!". But that is the risk trauma therapists take when they persuade their patients, on the basis of symptoms that might be implicit memories, that they were in fact traumatized. The general lack of independent corroboration is the Achilles’ heel in the trauma-memory argument.
In experimental psychology, of course, repression has had a vexed existence almost from the beginning. Researchers who have looked for repression in the laboratory have rarely found it, and even the few ostensibly positive findings are beset by a host of methodological problems (Holmes, 1974, 1990; MacKinnon & Dukes, 1964; Zeller, 1950). In the aftermath of seven decades of negative reviews, it was perhaps no oversight that the Handbook of Emotion and Memory did not even include a chapter on repression, and only six entries in the index (Christianson, 1992).
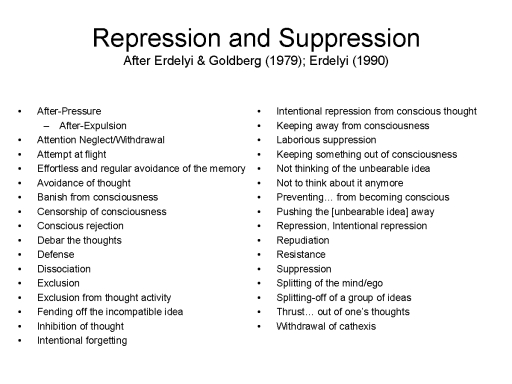 There is a further question about the
relationship between
repression (or dissociation, for that matter) and suppression or
denial. It is
one thing to deny that something happened, or to deliberately
avoid thinking
about something that did happen, and another thing entirely to
be unaware of
something that happened – or, for that matter, to be unaware
that one is
avoiding thinking about something that happened. Erdelyi has
vigorously argued
that Freud used the terms repression and suppression
interchangeably throughout his career, and referred to conscious
and unconscious
forms of repression. In Erdelyi’s view, the restriction of
repression to
unconscious defense was a later revisionist ploy by his daughter
Anna (Erdelyi,
1990; Erdelyi & Goldberg, 1979). Erdelyi’s philological
legwork is on
point, to be sure, but – as both Sigmund and Anna Freud surely
understood –
the concept of repression, and the technique of psychoanalysis,
only make sense
if repression is deployed unconsciously. Rapaport
(Rapaport, 1942) seems
to identify repression with unconscious defense; and if Wegner
(Wegner, 1989;
Wegner, Schneider, Carter, & White, 1987) is to be believed,
unconscious
thought suppression is the only kind of thought suppression that
can work
anyway. Conscious thought-suppression inevitably results in
ironic rebound.
There is a further question about the
relationship between
repression (or dissociation, for that matter) and suppression or
denial. It is
one thing to deny that something happened, or to deliberately
avoid thinking
about something that did happen, and another thing entirely to
be unaware of
something that happened – or, for that matter, to be unaware
that one is
avoiding thinking about something that happened. Erdelyi has
vigorously argued
that Freud used the terms repression and suppression
interchangeably throughout his career, and referred to conscious
and unconscious
forms of repression. In Erdelyi’s view, the restriction of
repression to
unconscious defense was a later revisionist ploy by his daughter
Anna (Erdelyi,
1990; Erdelyi & Goldberg, 1979). Erdelyi’s philological
legwork is on
point, to be sure, but – as both Sigmund and Anna Freud surely
understood –
the concept of repression, and the technique of psychoanalysis,
only make sense
if repression is deployed unconsciously. Rapaport
(Rapaport, 1942) seems
to identify repression with unconscious defense; and if Wegner
(Wegner, 1989;
Wegner, Schneider, Carter, & White, 1987) is to be believed,
unconscious
thought suppression is the only kind of thought suppression that
can work
anyway. Conscious thought-suppression inevitably results in
ironic rebound.
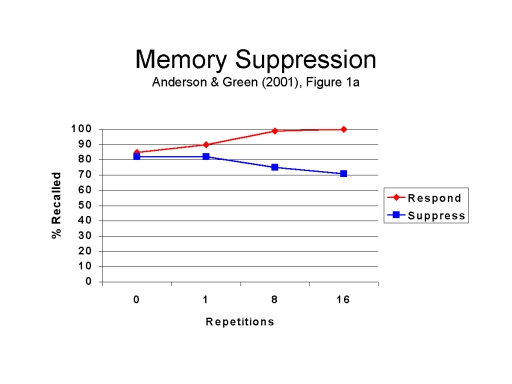 The point is important because directed
forgetting, a
variant on conscious thought suppression, has recently been
proposed as a model
of Freudian repression. In such experiments, subjects study a
list of items, and
then receive instructions to forget some of them, followed by
memory tests. The
general finding of such experiments is that instructions to
forget do seem to
work under some circumstances (Anderson & Green, 2001). This
much has long
been known (Bjork, 1972, 1978; Kihlstrom, 1983), but Anderson
and his
colleagues, as well as some other researchers, have repeatedly
referred to their
experimental results as relevant to Freud's views about the
repression of trauma
(Anderson & Levy, 2002; Conway, 2001; Levy & Anderson,
2002). However,
there are a large number of differences between Freudian
repression and directed
forgetting (Kihlstrom, 2002; see also Schacter, 2001). In the
first place, the
effect produced on explicit memory was nothing like a
full-fledged amnesia: even
after 16 suppression trials, the subjects still recalled more
than 70% of the
critical material. Moreover, the experiment provided no evidence
of a persisting
influence of unconscious (implicit) memory, or of the reversal
of the
"amnesia" and recovery of the lost memories – points that are
critical to the classical concept of repression. Most important,
however, even
the small effects observed are the product of conscious
thought
suppression – and conscious thought suppression cannot be a
model of
repression if repression must be unconscious.
The point is important because directed
forgetting, a
variant on conscious thought suppression, has recently been
proposed as a model
of Freudian repression. In such experiments, subjects study a
list of items, and
then receive instructions to forget some of them, followed by
memory tests. The
general finding of such experiments is that instructions to
forget do seem to
work under some circumstances (Anderson & Green, 2001). This
much has long
been known (Bjork, 1972, 1978; Kihlstrom, 1983), but Anderson
and his
colleagues, as well as some other researchers, have repeatedly
referred to their
experimental results as relevant to Freud's views about the
repression of trauma
(Anderson & Levy, 2002; Conway, 2001; Levy & Anderson,
2002). However,
there are a large number of differences between Freudian
repression and directed
forgetting (Kihlstrom, 2002; see also Schacter, 2001). In the
first place, the
effect produced on explicit memory was nothing like a
full-fledged amnesia: even
after 16 suppression trials, the subjects still recalled more
than 70% of the
critical material. Moreover, the experiment provided no evidence
of a persisting
influence of unconscious (implicit) memory, or of the reversal
of the
"amnesia" and recovery of the lost memories – points that are
critical to the classical concept of repression. Most important,
however, even
the small effects observed are the product of conscious
thought
suppression – and conscious thought suppression cannot be a
model of
repression if repression must be unconscious.
 Sincere attempts to study repression in
the laboratory have
often been rejected as irrelevant by psychoanalysts themselves.
Partly, this is
due to a methodological problem identified early on by Sears
(Sears, 1936) and
Rapaport (Rapaport, 1942): Repression is not about forgetting
the merely
unpleasant; It is about the forgetting of vital threat – threat
whose
intensity simply cannot be reproduced in the laboratory. Even
so, to
psychoanalysts, repression is obvious in their consulting rooms,
and
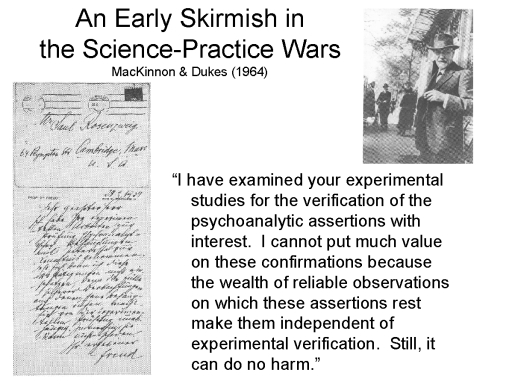
experimental evidence is not necessary. As Freud himself put it
in his 1934 note
to Saul Rosenzweig (MacKinnon & Dukes, 1964, p. 703):
Sincere attempts to study repression in
the laboratory have
often been rejected as irrelevant by psychoanalysts themselves.
Partly, this is
due to a methodological problem identified early on by Sears
(Sears, 1936) and
Rapaport (Rapaport, 1942): Repression is not about forgetting
the merely
unpleasant; It is about the forgetting of vital threat – threat
whose
intensity simply cannot be reproduced in the laboratory. Even
so, to
psychoanalysts, repression is obvious in their consulting rooms,
and
experimental evidence is not necessary. As Freud himself put it
in his 1934 note
to Saul Rosenzweig (MacKinnon & Dukes, 1964, p. 703):
I have examined your experimental studies for the verification of the psychoanalytic assertions with interest. I cannot put much value on these confirmations because the wealth of reliable observations on which these assertions rest make them independent of experimental verification. Still, it can do no harm.
 By contrast with repression, the concept
of dissociation has
fared somewhat better in its later history. As noted earlier,
Hilgard’s
neodissociation theory of divided consciousness was instrumental
in reviving
interest in the phenomenon. One important aspect of his work was
to show that
divisions of consciousness could occur in normal mental life,
without being
instigated by trauma. We see dissociative divisions of
consciousness all the
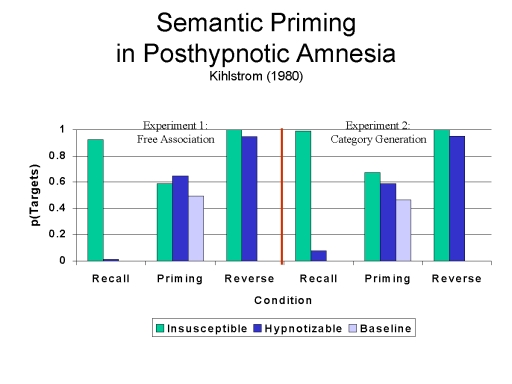
time in hypnosis, for example (Kihlstrom, 2004). In posthypnotic
amnesia, highly hypnotizable subjects cannot remember
what they did or experienced while they were hypnotized – yet
they show both
repetition and semantic priming effects related to those
experiences, revealing
a dissociation between explicit and implicit memory.
Furthermore, they recover
the critical memories when the amnesia suggestion is canceled by
a prearranged
reversibility cue. Spared priming is also observed in
hypnotically suggested
blindness, revealing a dissociation between explicit and
implicit perception.
Posthypnotic suggestion also has some of the character of
implicit learning: by
virtue of posthypnotic amnesia, subjects typically forget that
they received the
suggestion; yet they respond appropriately to the posthypnotic
cue.
By contrast with repression, the concept
of dissociation has
fared somewhat better in its later history. As noted earlier,
Hilgard’s
neodissociation theory of divided consciousness was instrumental
in reviving
interest in the phenomenon. One important aspect of his work was
to show that
divisions of consciousness could occur in normal mental life,
without being
instigated by trauma. We see dissociative divisions of
consciousness all the
time in hypnosis, for example (Kihlstrom, 2004). In posthypnotic
amnesia, highly hypnotizable subjects cannot remember
what they did or experienced while they were hypnotized – yet
they show both
repetition and semantic priming effects related to those
experiences, revealing
a dissociation between explicit and implicit memory.
Furthermore, they recover
the critical memories when the amnesia suggestion is canceled by
a prearranged
reversibility cue. Spared priming is also observed in
hypnotically suggested
blindness, revealing a dissociation between explicit and
implicit perception.
Posthypnotic suggestion also has some of the character of
implicit learning: by
virtue of posthypnotic amnesia, subjects typically forget that
they received the
suggestion; yet they respond appropriately to the posthypnotic
cue.
 Of course, the DSM category of
dissociative disorder
also indicates that the concept of dissociation has attained
general acceptance
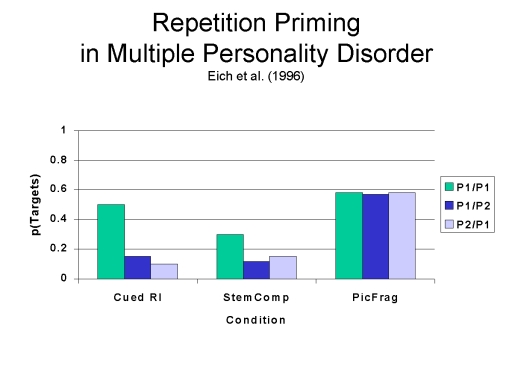
(Kihlstrom, 1992b, 1994). And again, we can see dissociations in
the
dissociative disorders. The interpersonality amnesia observed in
multiple
personality disorder, for example, impairs explicit memory but
spares at least
some forms of implicit memory (Eich, Macaulay, Lowewenstein,
& Dihle, 1997).
Still, we have to be careful here, because the term
"dissociation" can
be used in two quite different senses. Neuropsychologists use
the word in a
purely descriptive matter, to refer to a situation where a
single independent
variable has different effects on two dependent variables. When
we say that the
amnesic syndrome or posthypnotic amnesia dissociate explicit and
implicit
memory, we are using the term "dissociation" as a kind of
synonym for
statistical interaction. This usage goes back is at least to
William James
(James, 1890/1980), who coined the term to refer to a disruption
in the normal
association between two processes. It’s what Janet had in mind
when he
referred to désagrégation, translated as dissociation.
And it’s
also what DSM means, at least on the surface, when it
defines the
dissociative disorders as entailing disruptions in the normally
integrated
functions of consciousness.
Of course, the DSM category of
dissociative disorder
also indicates that the concept of dissociation has attained
general acceptance
(Kihlstrom, 1992b, 1994). And again, we can see dissociations in
the
dissociative disorders. The interpersonality amnesia observed in
multiple
personality disorder, for example, impairs explicit memory but
spares at least
some forms of implicit memory (Eich, Macaulay, Lowewenstein,
& Dihle, 1997).
Still, we have to be careful here, because the term
"dissociation" can
be used in two quite different senses. Neuropsychologists use
the word in a
purely descriptive matter, to refer to a situation where a
single independent
variable has different effects on two dependent variables. When
we say that the
amnesic syndrome or posthypnotic amnesia dissociate explicit and
implicit
memory, we are using the term "dissociation" as a kind of
synonym for
statistical interaction. This usage goes back is at least to
William James
(James, 1890/1980), who coined the term to refer to a disruption
in the normal
association between two processes. It’s what Janet had in mind
when he
referred to désagrégation, translated as dissociation.
And it’s
also what DSM means, at least on the surface, when it
defines the
dissociative disorders as entailing disruptions in the normally
integrated
functions of consciousness.
In either case, dissociation simply describes a situation where some percept, memory, or thought is not accessible to conscious awareness. But dissociation can also refer to a psychopathological process. This use of the term as an explanation, rather than a description, began appearing in the 1990s, as the dissociative disorders began to be viewed as syndromes of trauma. Thus, van der Kolk and others have argued that stress-induced increases in corticosteroids interfere with hippocampal function, and thus the storage of an explicit memory of the stressful event; but have no effect on the storage of implicit emotional associations, which is mediated by the amygdala (van der Kolk, 1994; van der Kolk & Fisler, 1993). As a result, trauma victims will respond emotionally to objects and events that somehow resemble the original trauma, without consciously remembering the trauma itself. In this usage, dissociation is an explanatory construct, not a descriptive label. Trauma causes dissociation, which renders the victim amnesic – an amnesia which in turn is characterized by dissociations between explicit and implicit memory.
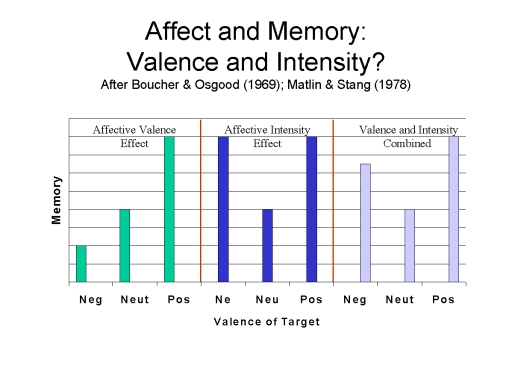 The only problem with this
assertion, which after all goes back
at least as far as Janet, is that everything we know about
emotion and memory
tells us that emotional involvement makes events more
memorable, not
less. At least, this is true in the mundane circumstances of the
affective
intensity effect familiar in laboratory studies of verbal
learning,
(Kihlstrom, Eich, Sandbrand, & Tobias, 2000). Of course,
higher levels of
stress, or different kinds of stress, might have different
effects. In this way,
proponents of the trauma-memory argument and recovered-memory
therapy often
argue that traumatic memories have special properties that
render the usual
rules of memory processing inapplicable.
The only problem with this
assertion, which after all goes back
at least as far as Janet, is that everything we know about
emotion and memory
tells us that emotional involvement makes events more
memorable, not
less. At least, this is true in the mundane circumstances of the
affective
intensity effect familiar in laboratory studies of verbal
learning,
(Kihlstrom, Eich, Sandbrand, & Tobias, 2000). Of course,
higher levels of
stress, or different kinds of stress, might have different
effects. In this way,
proponents of the trauma-memory argument and recovered-memory
therapy often
argue that traumatic memories have special properties that
render the usual
rules of memory processing inapplicable.
In 1997, Katherine Krause Shobe and I questioned whether traumatic memories were special, and concluded that the major theories of traumatic memory were either incoherent or inadequately supported by empirical evidence. For example, Terr’s distinction between punctate "Type I" and repeated "Type II" traumas (Terr, 1994) is based on an analysis that confounds the duration of the trauma with the age at which the trauma occurred. And Freyd’s distinction between the traumas of terror, which are well remembered, and traumas of betrayal, which are repressed and dissociated (Freyd, 1996), remains largely speculative.
In apparent response to our critique, Nadel and Jacobs took another tack to support the idea that traumatic memories are special (Nadel & Jacobs, 1998). According to them, different aspects of memories are processed by different memory modules. Furthermore, they argued that emotion, and particularly traumatic stress, affects the function of these memory modules differently. The differential effects of emotion on different memory modules provide the mechanism by which traumatized individuals can forget some aspects of their experiences but not others, resulting in the kinds of fragmentary memories described by van der Kolk and Fisler in a widely cited paper (van der Kolk & Fisler, 1995).
In support of the first proposition, Nadel and Jacobs cited a number of animal studies showing that "various aspects of an episode memory are represented and stored in dispersed neocortical modules" (p. 155), collected into a "hippocampal ensemble" (p. 155). As far as it goes, this view of the neural substrates of memory is unobjectionable. The distributed nature of memory processing -- in which, for example, emotional valence is contributed by the amygdala, recognition mediated by the rhinal cortex, spatial context by the parahippocampal gyrus, and the whole trace bound together by the hippocampal formation -- is widely accepted within cognitive neuropsychology and cognitive neuroscience.
In principle, the fact that different aspects of a memory are processed by different brain structures could provide the foundation for the fragmentary nature of emotional memory noted by van der Kolk and Fisler, among other proponents of the trauma-memory argument and recovered-memory therapy. If one module were impaired (for example, by the biological consequences of traumatic stress), the information processed by that module might well be missing from the resulting memory.
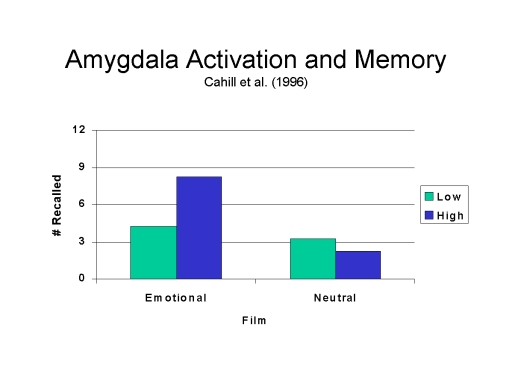 However, this proposition must be
considered purely
speculative, because Nadel and Jacobs offer no evidence in
support of the second
proposition, that the functioning of these cortical subsystems,
or the
representational components generated by them, are
differentially impaired by
traumatic stress. On the contrary, there are good reasons to
think that the
amygdala is activated by stress, resulting in robust, lasting
memory for
emotional events, as demonstrated convincingly by Cahill and his
colleagues
(Cahill, Prins, Weber, & McGaugh, 1994) , in widely known
research that
Nadel and Jacobs failed to cite (see also Cahill & McGaugh,
1996, 1998;
McGaugh, 2004). The trauma-memory argument seeks to explain why
people forget
trauma; it cannot be supported by evidence that the involvement
of the amygdala
makes events more memorable.
However, this proposition must be
considered purely
speculative, because Nadel and Jacobs offer no evidence in
support of the second
proposition, that the functioning of these cortical subsystems,
or the
representational components generated by them, are
differentially impaired by
traumatic stress. On the contrary, there are good reasons to
think that the
amygdala is activated by stress, resulting in robust, lasting
memory for
emotional events, as demonstrated convincingly by Cahill and his
colleagues
(Cahill, Prins, Weber, & McGaugh, 1994) , in widely known
research that
Nadel and Jacobs failed to cite (see also Cahill & McGaugh,
1996, 1998;
McGaugh, 2004). The trauma-memory argument seeks to explain why
people forget
trauma; it cannot be supported by evidence that the involvement
of the amygdala
makes events more memorable.
Nadel and Jacobs do cite a number of animal studies showing that increased stress impairs hippocampal functioning, and thus memory. But the stress in question is chronic stress (e.g., 21 days of restraint), and the memory task in question is unrelated to the stressful event (e.g., maze learning). It is highly plausible, as Sapolsky (1998) has suggested, that exposure to chronic stress releases neurotoxins which damage the hippocampus and consequently impair memory. But this memory impairment would be general in nature, not specific to the trauma, and would include memories unrelated to the trauma. The amnesia would be anterograde in nature, not including the initial trauma itself (the retrograde effects of hippocampal damage remain highly controversial). And it would be progressive, producing denser amnesic lacunae as the stress continued. There is no evidence from controlled research on either humans or animals that stress specifically impairs memory for the central details of the stressful event itself -- which is what the claim of "repressed" or "dissociated" traumatic memories is all about. Holocaust survivors do not forget the Holocaust.
Nadel and Jacobs' third proposition, that traumatic memory is fragmentary, is the outcome to be explained by the first two propositions. But if the second of these propositions is invalid, what is there to be said about the third? In fact, Nadel and Jacobs seem to base their third proposition entirely on the work of van der Kolk and Fisler (van der Kolk & Fisler, 1995):
Within a certain range, stress could enhance all forms of explicit memory, but high levels of stress could enhance some aspects of explicit memory while impairing others. And here is the critical point: When stress is high enough to impair the function of the hippocampus, resulting memories will be different from those formed under more ordinary circumstances. These empirical data may be available as isolated fragments rather than as coherently bound episodes (e.g., van der Kolk & Fisler, 1995). This hypothesis contrasts with the position espoused by Shobe and Kihlstrom (1997), who did not take into account the differential effects of stress on the various memory modules (p. 156).
Note, first, that the material quoted is presented only as a "hypothesis", and it is qualified with hedge words such as "could" and "may". In fact, nowhere in their paper do Nadel and Jacobs offer any evidence that stress has the predicted effect on memory; it is not clear why they should criticize us for failing to take into account evidence that did not exist at the time, and apparently still does not exist.
It is ironic that, in bolstering their "hypothesis" concerning the fragmentary nature of traumatic memories, Nadel and Jacobs rely heavily on van der Kolk and Fisler (1995), because -- as Shobe and I discussed in some detail – this study is badly confounded, and no conclusions about the qualities of traumatic memory should be drawn from it. These investigators recruited subjects for their study by advertising in a local newspaper for individuals who were "haunted by memories of terrible life experiences" (p. 514), which they then compared to self-selected memories for events such as weddings and graduations. To make things worse, most of the traumatic events were reported to have occurred in childhood, while most of the nontraumatic events occurred in adulthood. As Shobe and I wrote: "the poor narrative quality of the traumatic memories, and even the periods of amnesia, may have been due to normal processes associated with infantile and childhood amnesia, rather than any special qualities of traumatic memory (Shobe & Kihlstrom, 1997, p. 72). Yet Nadel and Jacobs accept van der Kolk and Fisler's evidence uncritically.
Nadel and Jacobs attempt to bolster their position further by citing an earlier paper by Jacobs, Laurence, Thomas, Luzcak, and Nadel as supporting the notion that "even in the presence of extensive autobiographical amnesia, intrusive emotions or images associated with the trauma (and related events) may appear" (Jacobs, Laurance, Thomas, Luzcak, & Nadel, 1996, p. 156; see lso Thomas, Laurance, Jacobs, & Nadel, 1995). Unfortunately, the paper in question (which they misreference) presents no empirical data to support this or any other notion about traumatic memory. Instead, these authors offer yet another hypothesis about "the conditions under which a memory for a traumatic event has a high, medium, or low probability of accurately reflecting the target event", as well as a series of fictional (sic) cases illustrating the basic points of the proposed model. This hypothesis was not tested in the Jacobs et al. (1996), paper, and as such remains highly speculative. Nevertheless, Nadel and Jacobs conclude their discussion as if the model had been supported by empirical data: "What distinguishes these intrusive memory states is the absence of the time-and-place contextual information that typically characterizes autobiographical episode memory" (p. 156).
In further support of their arguments, Nadel and Jacobs cited a paper by Metcalfe and Jacobs (see also Metcalfe & Jacobs, 1996; Metcalfe & Jacobs, 1998; Metcalfe & Jacobs, 2000) which proposes that there are separate "cool" and "hot" memory systems which are affected differently by stress. Metcalfe and Jacobs propose that:
"As stress increases, the cool-memory system at first becomes increasingly responsive but then, as the level continues to grow, becomes less responsive until, at traumatic levels, of stress, it becomes dysfunctional.... In contrast, the hot system becomes increasingly responsive to increasing levels of stress in a monotonic manner up to and including very extreme levels, breaking down only at extremely high levels" (pp. 205-206).
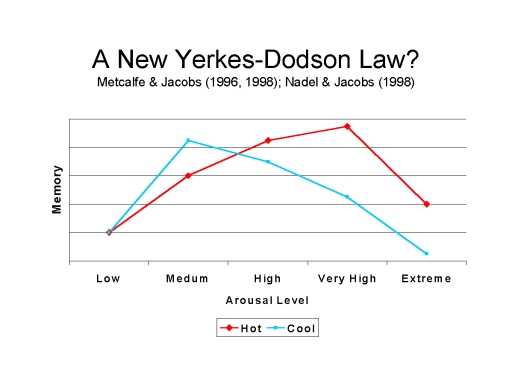 Like Nadel and Jacobs, Metcalfe and Jacobs
seem to be invoking
something like the Yerkes-Dodson Law, the famous
inverted-U-shaped function that
relates arousal to performance (Yerkes & Dodson, 1908).
According to the
law, there is some moderate level of arousal that leads to
optimum performance.
Extremely high levels of arousal impair performance, perhaps by
activating
competing responses that are ordinarily inhibited, or perhaps by
reducing the
number of cues that the organism can process (Easterbrook,
1959). Either way
high levels of arousal might produce just the kinds of
fragmentary memories
described by van der Kolk and Fisler. But fragmentary memory is
not the absence
of memory. High levels of arousal might impair the victim’s
memory for
peripheral details, but there is no reason to think they might
impair memory for
central details, like the event itself. Moreover, even if high
levels of arousal
impaired the processing of central as well as peripheral
details, the massive
encoding failure would render attempts to recover traumatic
memories pointless:
there would be no traumatic memory available to recover.
Like Nadel and Jacobs, Metcalfe and Jacobs
seem to be invoking
something like the Yerkes-Dodson Law, the famous
inverted-U-shaped function that
relates arousal to performance (Yerkes & Dodson, 1908).
According to the
law, there is some moderate level of arousal that leads to
optimum performance.
Extremely high levels of arousal impair performance, perhaps by
activating
competing responses that are ordinarily inhibited, or perhaps by
reducing the
number of cues that the organism can process (Easterbrook,
1959). Either way
high levels of arousal might produce just the kinds of
fragmentary memories
described by van der Kolk and Fisler. But fragmentary memory is
not the absence
of memory. High levels of arousal might impair the victim’s
memory for
peripheral details, but there is no reason to think they might
impair memory for
central details, like the event itself. Moreover, even if high
levels of arousal
impaired the processing of central as well as peripheral
details, the massive
encoding failure would render attempts to recover traumatic
memories pointless:
there would be no traumatic memory available to recover.
Still, even the assertion of a new Yerkes-Dodson Law takes the form of a hypothesis. Metcalfe and Jacobs (1998) review available evidence that low levels of stress can enhance processing of both the "cool" (hippocampus-based) and "hot" (amygdala-based) memory systems, as well as available evidence that moderate levels of stress can enhance "hot" memory while impairing "cool" memory to some degree. However, they offer no evidence for the critical prediction that traumatic stress can produce profound amnesia for the spatio-temporal components of memory processed by the "cool" system. Aside from two anecdotal case reports of unknown representativeness, Metcalfe and Jacobs rely entirely on the study by van der Kolk and Fisler (1995) -- the same study that Shobe and I had already criticized in considerable detail.
It is important to understand precisely what is going on here. Nadel and Jacobs offer no empirical support for their prediction that individuals subjected to traumatic levels of stress can retain strong memories for their emotional state while forgetting the spatio-temporal context in which this emotion was aroused. Although they refer to the papers by Jacobs et al. (1996) and Metcalfe & Jacobs (1998) as if they presented such evidence, these papers both rely solely on the highly questionable study by van der Kolk and Fisler (1995). As such, their hypothesis remains just that -- a hypothesis that has no grounding in actual empirical data.
A hypothesis (Nadel & Jacobs, 1998) cannot be supported merely by repetitions of the same hypothesis in other publications (Jacobs et al., 1996; Metcalfe & Jacobs, 1998).
Despite the lack of pertinent evidence, Nadel and Jacobs (1998) concluded that "Traumatic stress can cause amnesia for the autobiographical context of stressful events, but stronger than normal recall for the emotional memories produced by them" (p. 156). But they went even further, concluding that despite the allegedly fragmentary nature of traumatic memories, "an autobiographical memory eventually emerges" by a process of "'inferential narrative smoothing' whereby disembodied fragments are knit together into a plausible autobiographical episode.... The present analysis suggests that at least some memories 'recovered' during therapy should be taken seriously" (p. 156).
The evidence provided that memory fragments can be knitted into autobiographical narratives is, once again, the study by van der Kolk and Fisler (1995). Unfortunately, these authors did not attempt to corroborate their subjects' narratives against independent records of the traumatic events in question. Accordingly, we have no idea how much of their subjects' narratives were accurate accounts of the traumatic events in question -- or, frankly even that the events occurred at all. In fact, Nadel and Jacobs concede that "The narratives associated with [recovered traumatic] memories are less likely to be veridical in their entirety" (p. 156). Given that, according to their own hypothesis, the contextual information underlying these narratives was not properly encoded at the time the events ostensibly occurred, this would seem to be an understatement.
Six years later, Jacobs, Nadel, and their colleagues repeated essentially the same argument (Payne, Nadel, Britton, & Jacobs, 2004). Once again, they conflated memory and cognitive difficulties that might be caused by the neurotoxic effects of chronic stress with traumatic amnesia mediated by repression or dissociation. Once again, they relied on the van der Kolk and Fisler study for evidence that "traumatic events are remembered initially as disconnected images and waves of disjointed sensations" (p. 97) – plus a description of a "hypothetical traumatic war experience" (p. 95). Once again, they proposed that "If high levels of cortisol disrupt normal neuronal function... [of the hippocampus], then coherent memories of trauma will be rendered inaccessible. This time, at least, the proposal by Metcalfe and Jacobs of two memory systems, one hot and one cool, is clearly labeled "speculative" (p. 98), and the notion of traumatic amnesia is acknowledged to be "controversial" (p. 113). Nevertheless, these authors conclude that "Intense stress is associated with memory disruption, either partial or complete, relating to the trauma itself or to episodic memory in general" (p. 102), and that "Trauma appears to disrupt memory for the context and the details of experienced events" (p. 111).
In the final analysis, Nadel and Jacobs attempt to support their proposition that traumatic memory is special by offering little more than an unproven "hypothesis" about why this should be so. Although the theoretical basis for their prediction is clear, empirical evidence that trauma actually causes amnesia is lacking in their paper, and indeed in the wider body of evidence on emotion and memory. Nor does even their own hypothesis give us any reason to have any confidence in traumatic narratives "recovered" through psychotherapy. It may well be that traumatic memory is special in the ways asserted by Nadel and Jacobs, but for the present we have only their word for it. And, frankly, all the evidence appears to be to the contrary.
Admittedly, much of the literature on the effects of very high levels of stress is animal literature, and studies of animal memory are often open to interpretation as pertaining to implicit, or at least nonverbal, memories. Nevertheless, under this gambit the very literature that Cahill and McGaugh cite as evidence that stress improves memory can be cited in favor of the trauma-memory argument, on the assumption that high levels of stress impair the encoding of explicit, consciously accessible memories of the sort that might be expressed in free recall, but enhance the encoding of implicit, unconscious ones that might be expressed in priming and other aspects of behavior. Of course, such a reconstrual risks confusing unconscious implicit memories with conscious explicit memories that are simply nonverbal in nature. Setting this nontrivial problem aside, in the final analysis, it all comes down to a simple question: is there any evidence that psychological trauma actually causes functional or psychogenic amnesia – that is, a profound loss of explicit memory for traumatic and peritraumatic events?
Although traumatic amnesia has been part of the folklore of psychiatry and clinical psychology since the 19th century (Janet and Freud both made it a central part of their theories of neurosis and psychotherapy), the best that can be said is that after more than 100 years even the best evidence favoring the existence of traumatic amnesia is highly debatable (Crews, 1995, 2004). Even amnesia in war neurosis – perhaps the prototype of stress-induced functional amnesia (Brown, Scheflin, & Hammond, 1998) – rests on an unsecure empirical base. As Pendergrast (Pendergrast, 1998) has pointed out, the classic monographs of Kardiner and Spiegel (Kardiner & Spiegel, 1941/1947) and Grinker and Spiegel (Grinker & Spiegel, 1943/1945) each include only a single detailed case report of traumatic amnesia (for detailed critiques of the war neurosis literature, see also Giglio, 1998; Lilienfeld & Loftus, 1998; Piper, 1998). Amnesia may occasionally occur in the context of war neurosis, but apparently it does not happen often enough to permit clinicians who were actively looking for it to report a series of cases. Moreover, as Pendergrast also pointed out, the general failure of clinicians to independently corroborate memories of war-related trauma recovered through such means as hypnosis and the amytal interview (e.g., Fisher, 1945) raises the possibility that many, if not most, of these memories are confabulations.
In view of the problem of obtaining independent corroboration of retrospective reports of trauma, it would seem that the best evidence for trauma-induced amnesia would be provided by prospective studies of actual trauma survivors. In a comprehensive review of the available literature, Pope and his colleagues surveyed 63 studies of more than 10,000 trauma survivors, everything from the Holocaust and war to accidents and natural disasters, and concluded that they recorded "not a single instance" of a psychogenic amnesia caused by processes such as repression or dissociation (Pope, Hudson, Bodkin, & Oliva, 1998, p. 213). Most victims apparently remembered their experiences all too well. Those who did not could be accounted for by organic amnesia, or by normal memory processes such as infantile and childhood amnesia or time-dependent forgetting (Pope, Oliva, & Hudson, 2000).
By contrast, Brown and his colleagues reviewed much of the same literature in book of almost 800 pages, leading toward quite the opposite conclusion (Brown et al., 1998). For example, they concluded that "A significant subpopulation of traumatized individuals retain no or little narrative memory for the trauma" (p. 200). Although the exigencies of publication prevented Brown and his colleagues from confronting Pope’s analysis directly, they did so in a further paper, more than 150 pages long, just the next year (Brown, Scheflin, & Whitfield, 1999). After rejecting 42 of the 63 studies as "irrelevant" to the question of amnesia, Brown et al. (1999) concluded that "all 21 [of the remaining studies] show that trauma significantly affected memory – and 18 demonstrate amnesia either for the traumatic event or for injuries related to the trauma" (p. 29). As it happens, the 21 allegedly positive studies were a mixed bag, including evidence for general memory disturbance of the sort often seen in PTSD, or for "cognitive avoidance" of the trauma, rather than amnesia per se. But Brown et al. did assert that "Nine studies actually present data in favor of the existence of traumatic amnesia" (p. 28, emphasis added).
In response, Piper and his colleagues re-analyzed those nine studies and reaffirmed the conclusions of Pope et al (see also McNally, 2003; Piper, Pope, & Borowiecki, 2000). For example, two individuals who were amnesic for a lightning strike were "side-flash" victims who probably received the equivalent of electroconvulsive shock. Some of the children who forgot a flood disaster were as young as two years old at the time of the incident. And while approximately one-third of older children who were earthquake survivors were reported as showing psychogenic amnesia for the event, more than two-thirds of a control group of children who were not directly exposed to the trauma met the same criterion. One study did report a high rate of dissociative symptoms, as measured by the DES, among those who experienced the Loma Prieta earthquake of 1989, but these were most likely common experiences of depersonalization and derealization; there was no evidence that any subject forgot the earthquake.
In the face of such evidence, the trauma-memory argument is sometime revised to take special note of trauma associated with incest and other childhood sexual abuse (Brown et al., 1998; Scheflin & Brown, 1996). For example, Freyd has proposed that traumas of terror, such as natural disasters, are remembered well, while traumas of betrayal, such as incestuous sexual abuse, are dissociated from conscious recollection. Brown and his colleagues reviewed the literature on "naturally occurring dissociative or traumatic amnesia for childhood sexual abuse", and concluded that "Not a single one of the 68 data–based studies failed to find it" (Brown et al., 1999, p. 127)(see also p. 67).
Unfortunately, these studies suffer from a host of methodological problems, including, in many cases, an unhealthy reliance on self-reports -- both that the trauma in question actually occurred, and that it was actually forgotten (Kihlstrom, 1996, 1998; Loftus, Garry, & Feldman, 1994; Pendergrast, 1996; Harrison G. Pope & James I. Hudson, 1995). Even where there is independent verification of the abuse, there is often a failure to distinguish between amnesia and the normal forgetting that occurs with the passage of time – not to mention infantile and childhood amnesia. Typically, there is also a failure to distinguish between actual forgetting and failures of self-disclosure. For example, Brown et al. (Brown et al., 1998) cited a massive study by Widom and Morris (Widom & Morris, 1997) of "full amnesia" in 37% of 1,114 adult survivors of "court-substantiated" childhood sexual abuse (p. 196) – despite the fact that Widom and Morris themselves specifically disavowed such an interpretation, and attributed their reporting failures as lack of disclosure rather than amnesia. In view of these problems, perhaps a more accurate statement would be that not a single one of the studies in question convincingly showed it.
 When researchers take account of these
sorts of factors, the
incidence of "amnesia" for child abuse goes way down. In a study
of
victims of documented child sexual abuse (CSA), Gail Goodman and
her colleagues
reported that only 15.5% of abuse victims failed to report the
target incident
during a telephone interview conducted an average of 13 years
after the events
in question (Goodman et al., 2003). Nondisclosure dropped to
8.3% after
follow-up by a mailed questionnaire and a telephone interview.
Both rates of
reporting failure are markedly lower than that yielded by
earlier, less rigorous
studies (e.g., Williams, 1994).
When researchers take account of these
sorts of factors, the
incidence of "amnesia" for child abuse goes way down. In a study
of
victims of documented child sexual abuse (CSA), Gail Goodman and
her colleagues
reported that only 15.5% of abuse victims failed to report the
target incident
during a telephone interview conducted an average of 13 years
after the events
in question (Goodman et al., 2003). Nondisclosure dropped to
8.3% after
follow-up by a mailed questionnaire and a telephone interview.
Both rates of
reporting failure are markedly lower than that yielded by
earlier, less rigorous
studies (e.g., Williams, 1994).
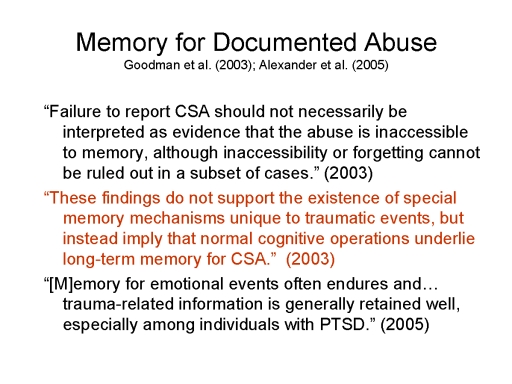
Although an 8% disclosure failure might be interpreted in terms of traumatic amnesia, it should be understood that this figure represents an upper limit, because the failure to report may for reasons other than repression or dissociation. Goodman’s detailed analysis support more prosaic interpretations in terms of infantile and childhood amnesia, depth of processing, time-dependent forgetting, and a simple unwillingness to disclose personal tragedy to a stranger. Accordingly, Goodman et al. concluded:
These findings do not support the existence of special memory mechanisms unique to traumatic events, but instead imply that normal cognitive operations underlie long-term memory for CSA (p. 117).
Goodman (this volume) has provided a further analysis of this data which provides further evidence against the trauma-memory argument. When directly questioned, 21 of the 142 respondents who completed the telephone interview reported that there had been some period of time when they had forgotten about the abuse. Of these, most engaged in conscious suppression: only 5 of 138 subjects who answered the question indicated that they would not have remembered the target incident if they had been asked directly about it, and a sixth was not sure – yielding a reduced estimate of 3.6% for the incidence of traumatic amnesia.
Although this estimate is an order of magnitude below Williams’ figure of 38%, it should be underscored that even this vastly reduced estimate is an upper bound. Goodman and her colleagues have reported that at least two of these subjects were very young at the time the target incident occurred – again raising the likelihood of infantile and childhood amnesia. Another victim was asleep at the time of the incident, and thus was not even aware of it at the time it occurred. That leaves only two individuals, at most 1.5% of the sample, who might conceivably have suffered from traumatic amnesia. Again, this figure is far below the figures given, suggested, or implied by proponents of the trauma-memory argument. For all we know, this level of co-occurrence of trauma and amnesia might be nothing more than sheer coincidence. In any event, the estimate is so low as to refute the claim, or implication, that trauma causes amnesia with anything like the regularity claimed by advocates of the trauma-memory argument and recovered-memory therapy.
Slide 37. Sometimes, recovered memories of abuse and other trauma are offered as evidence of repression or dissociation (Brown et al., 1998; Gleaves, smith, Butler, & Spiegel, 2004; Kihlstrom, 2004b). It is a telling point that, more than a century after the emergence of the trauma-memory argument, the most convincing evidence that its promulgators can offer are individual cases of doubtful generality. And even these are precious few in number, far between – and often of doubtful validity. For example, Karon and Widener offered, as an example of repression in battlefield neurosis, the case of a World War II veteran who had apparently repressed an airplane crash in which he rescued the pilot and earned a medal for his bravery (Karon & Widener, 1997, 1998). But it is not at all clear whether the episode actually represented the lifting of amnesia, as opposed to the patient’s more causal report that he had once received a medal (for detailed critiques, see Lilienfeld & Loftus, 1998; Pendergrast, 1998; Piper, 1998). Although there are serious questions about whether this recovered memory is accurate (Giglio, 1998; for a reply, see Karon & Widener, 1998), the fact remains that Karon and Widener did not even corroborate the one absolutely confirmable detail – that the patient in question did, in fact, receive a medal for bravery.
Other reported cases of recovered memory suffer from similar problems. For example, Cheit claimed to have validated 35 cases of recovered memory of child sexual abuse (Cheit, 1998), only to have the claim systematically dismantled by Piper (for a reply, see Cheit, 1999; Piper, 1999). Corwin and Olafson presented the case of Jane Doe, whose recovery of a memory of childhood sexual abuse was actually captured on videotape (Corwin & Olafson, 1997). Although this case study was compelling to many (if not all) researchers who were asked to comment on it, closer scrutiny raises the question of whether the subject in question recovered a memory of abuse, or only a memory of her previous testimony about abuse. The difference is critical – especially since the victim in question was the object of a vigorous custody dispute between divorcing parents, and there are serious questions about whether any abuse actually took place at all (Loftus & Guyer, 2002a, 2002b).
With respect to trauma and memory, the argument seems to be that because repression and dissociation can be reversed in theory, the recovery of memories shows that they were repressed or dissociated in the first place. At first blush, this would seem to be a textbook example of the logical fallacy of affirming the consequent: If repressed memories can be recovered, then recovered memories were repressed. But the recovery of a traumatic memory, even one that is independently corroborated (Schooler, 2001), does not by itself imply that the event was forgotten due to repression or dissociation. Researchers must be careful to distinguish between recoveries mediated by the lifting of repression or breaching of dissociation from other causes of remembering, including the normal effects of shifting retrieval cues, reminiscence effects, and hypermnesia. The recovery of a forgotten trauma may be no different in kind that the recovery of one’s memory for where one put the car keys, or the name of one’s third-grade teacher. It is also important to distinguish between the recovery of a forgotten memory of trauma and a reinterpretation of an event that had always been remembered. In any event, it should surprise no one if traumatic events are occasionally forgotten, and if recovered memories of trauma are occasionally corroborated. Neither empirical fact demands interpretation in terms of trauma-induced repression or dissociation.
Sometimes, proponents of the trauma-memory argument point to the existence of the dissociative disorders as evidence that trauma can be repressed, or dissociated, and thus lost to conscious recollection. As was the case with recovered memories, the argument verges on the circular: dissociative disorders exist, dissociative disorders are instigated by trauma, therefore trauma causes dissociative amnesia. Moreover, the argument seems to confuse the two meanings of the term dissociation discussed earlier: the dissociative disorders are "dissociative" in the descriptive sense of entailing a loss of the integrative functions of consciousness, and not because they are caused by stress-induced "dissociation". It is in this descriptive sense that the conversion disorders can also be described as dissociative in nature, although the dissociations in question affect sensory-perceptual and motor functioning, rather than memory (Kihlstrom, 1992b, 1994).
In fact, dissociative disorder is a valid diagnostic category (Kihlstrom, 2004a) and functional amnesia a genuine phenomenon (Kihlstrom & Schacter, 2000; see also Kopelman, 2002; Markowitsch, 2000) – although genuine cases appear to be vanishingly rare. Thigpen and Cleckley, who treated and reported the famous Three Faces of Eve (Thigpen & Cleckley, 1954; Thigpen & Cleckley, 1957), never saw another valid case despite repeated referrals over the next 30 years – even at the height of the multiple personality "epidemic" (Thigpen & Cleckley, 1984). Given the apparent incidence of child sexual abuse, if the trauma-memory argument – and particularly arguments about betrayal trauma (Freyd, 1996) – were correct, we should see more cases of dissociative amnesia than we do.
Although there are undoubtedly some cases of dissociative disorder who present histories of trauma, including incestuous child abuse, apparently this is not always, or even often the case. For example, the eponymous Eve denied ever having been abused, and complained that people who attended her speaking engagements insisted that she was in denial about having been abused (Ganaway, 1995). Even when a patient with dissociative disorder presents a documented history of child sexual abuse inferring a causal link between abuse and dissociation is fraught with difficulty (H.G. Pope & J.I. Hudson, 1995; Rind, 2003; Sbraga & O'Donohue, 2003). For example, the most widely cited evidence for an association between child sexual abuse and dissociative amnesia is retrospective in nature, and retrospective studies by their very nature necessarily overestimate the relation between antecedent and consequent variables (Dawes, 1993; Swets, Dawes, & Monahan, 2000). Moreover, such studies often rely on excessively liberal definitions of abuse and trauma to begin with.
In point of fact, there is actually no good evidence that trauma plays a particular role in the etiology of these disorders – that is, evidence based on random or prospective samples (Kihlstrom et al., 2000). In such studies, the fact is that example, multiple personality disorder and other dissociative disorders simply do not figure prominently among the sequelae of documented child sexual abuse (see also Bailey & Shriver, 1999; Beitchman, Zucker, Hood, & DaCosta, 1991, 1992; Kendall-Tackett & Marshall, 1998; Kendall-Tackett, Williams, & Finkelhor, 1993; Lange et al., 1999; Rind, Tromovich, & Bauserman, 1998). The dissociative disorders cannot be cited as evidence that trauma impairs memory unless, and until, there is convincing evidence that such traumas as child sexual abuse actually cause dissociative disorder. Occasional cases of dissociative disorder who also have a history of trauma have helped keep the trauma-memory argument alive. But even then they are the exceptions that test, one might go so far as to say prove, the rule that emotion – even negative emotion, even at extremely high levels – generally enhances memory, such that trauma is typically remembered particularly well by those who have actually experienced it.
A word is in order about the distinction between "organic" and "functional" (or "somatogenic" and "psychogenic" amnesia and other mental disorders. In medicine, the term "functional" often means that the biological basis of a disorder is not yet known, and there is no necessary implication that the disorder has no organic basis. For example, general paresis, a form of dementia, was considered functional until the discovery of the syphilis spirochete, at which point the illness was reclassified from functional to organic. On the other hand, the term "psychogenic" implies that the underlying etiology is psychological rather than biological in nature. Some forms of depression may reflect anomalies of neurotransmitter function, and thus properly classified as somatogenic in nature. On the other hand, other forms of depression may be considered psychogenic because they are caused by certain beliefs held by the patient – the "depressogenic" schemata of Beck (Beck, 1967), perhaps, or the pessimistic attributional style that lies at the core of the reformulated hopelessness theory (Abramson, Metalsky, & Alloy, 1989).
The memory disorder envisioned by the trauma-memory argument is, in theory, both functional and psychogenic. Traumatic amnesia is "functional" in that it "is attributable to an instigating event or process that does not result in damage to brain structures, and produces more forgetting than would normally occur in the absence of the instigating event or process" – in this case, trauma (Kihlstrom & Schacter, 2000, p. 409). And it is "psychogenic" in that it is caused by a mental state, namely mental trauma -- or mental processes of repression or dissociation.
The fact that dissociative amnesia might have biological correlates (Markowitsch, 1999) does not mean it is really "organic" in nature after all: it is axiomatic in contemporary psychology and cognitive science that all mental states have their neural correlates, and this is no less true for dissociative amnesia than it is for conscious recollection. What makes dissociative amnesia functional, at least in principle, is the absence of demonstrable brain insult, injury, or disease as an instigating factor. There are many other disorders of memory that are functional in just the same way (John F. Kihlstrom & Frederick J. Evans, 1979). These include posthypnotic amnesia, which is also psychogenic, because it only occurs in response to suggestion (Kihlstrom, 1985; Kihlstrom, 2004, in press; J.F. Kihlstrom & F. J. Evans, 1979). But the category also includes infantile and childhood amnesia, which is not psychogenic
By contrast, the memory dysfunction commonly associated with PTSD is "organic", because it is (ostensibly) caused by a stress-induced "glucocorticoid cascade" (Bremner, 2002; O'Brien, 1997) that damages the hippocampus; but it is also "psychogenic", because stress is defined psychologically by the experience of unpredictable and/or uncontrollable events (Mineka & Kihlstrom, 1978). To be clear: a functional amnesia is one that is not associated with brain insult, injury, or disease; a psychogenic amnesia has a mental, as opposed to an organic cause. The two categories overlap, but they are different.
The trauma-memory argument and recovered-memory therapy have been with us for more than 100 years, and have embedded themselves deeply into both our professional practices and our wider culture. But there was never any good evidence for either, and there still is none. Maybe such evidence will be forthcoming in the future. There are occasional cases in which traumatic stress and amnesia seem to go together, inviting interpretations in terms of repression or dissociation. But nothing in the case literature justifies assertions that trauma impairs memory as a matter of course, or in the majority of cases or often – even sometimes seems too extreme. In view of the paucity of evidence that trauma causes amnesia, discussion of implicit memories of trauma seems pointless. Laboratory analogs of traumatic amnesia are models in search of a phenomenon; theories of traumatic amnesia are explanations in search of facts.
Abramson, L. Y., Metalsky, G. I., & Alloy, L. B. (1989). Hopelessness depression: A theory-based subtype of depression. Psychological Review, 96, 358-372.
Alexander, K. W., Quas, J. N., Goodman, G. S., Ghetti, S., Edelstein, R. S., Redlich, A. D., Cordon, I. M., & Jones, D. P. H. (2005). Traumatic impact predicts long-term memory for documented child sexual abuse. Psychological Science, 16, 33-40.
Anderson, M. C., & Green, C. (2001). Suppressing unwanted memories by executive control. Nature, 410(15 March), 366-369.
Anderson, M. C., & Levy, B. (2002). Repression can (and should) be studied empirically. Trends in Cognitive Sciences, 6, 502-503.
Bailey, J. M., & Shriver, A. (1999). Does childhood sexual abuse cause borderline personality disorder. Journal of Sex and Marital Therapy, 25, 45-57.
Bass, E., & Davis, L. (1988). The courage to heal: A guide for women survivors of child sexual abuse. New York: Harper & Row.
Beck, A. T. (1967). Depression: Causes and treatment. Philadelphia: University of Pennsylvania Press.
Beitchman, J. H., Zucker, K. J., Hood, J. E., & DaCosta, G. A. (1991). A review of the short-term effects of child sexual abuse. Child Abuse & Neglect, 15(4), 537-556.
Beitchman, J. H., Zucker, K. J., Hood, J. E., & DaCosta, G. A. (1992). A review of the long-term effects of child sexual abuse. Child Abuse & Neglect, 16(1), 101-118.
Bjork, R. A. (1972). Theoretical implications of directed forgetting. In Melton & Martin (Eds.) (pp. 217-).
Bjork, R. A. (1978). The updating of human memory. In G. H. Bower (Ed.), The psychology of learning and motivation (pp. 235-259): Academic.
Bliss, E. L. (1986). Multiple personality, allied disorders, and hypnosis. New York: Oxford.
Blume, E. S. (1990). Secret survivors: Uncovering incest and its aftereffects on women. New York: Wiley.
Boor, M. (1982). The multiple personality epidemic: Additional cases and inferences regarding diagnosis, etiology, dynamics, and treatment. 170, 302-304.
Bremner, J. D. (2002). Does stress damage the brain? Understanding trauma-related disorders from a mind-body perspective. New York: Norton.
Breuer, J., & Freud, S. (1893-1895/1953). Studies on hysteria. (Vol. 2). London: Hogarth.
Brown, D., Scheflin, A. W., & Hammond, D. C. (1998). Memory, trauma treatment, and the law. New York: W.W. Norton.
Brown, D., Scheflin, A. W., & Whitfield, C. L. (1999). Recovered memories: The current weight of the evidence in science and in the courts. Journal of Psychiatry & Law, 27, 5-156.
Cahill, L., & McGaugh, J. L. (1996). Modulation of memory storage. Current Opinion in Neurobiology, 6, 237-242.
Cahill, L., & McGaugh, J. L. (1998). Mechanisms of emotional arousal and lasting declarative memory. Trends in Neurosciences, 21, 294-299.
Cahill, L., Prins, B., Weber, M., & McGaugh, J. L. (1994). Beta-adrenergic activation and memory for emotional events. Nature, 371, 702-704.
Cheit, R. E. (1998). Consider this, skeptics of recovered memory. Ethics & Behavior, 8, 141-160.
Cheit, R. E. (1999). Junk skepticism and recovered memory: A reply to Piper. Ethics & Behavior, 9, 295-318.
Christianson, S.-A. (Ed.). (1992). Handbook of emotion and memory: Research and theory. Hillsdale, N.J.: Erlbaum.
Conway, M. A. (2001). Repression revisited. Nature, 410, 319-320.
Corwin, D. L., & Olafson, E. (1997). Videotaped discovery of a reportedly unrecallable memory of child sexual abuse: comparison with a childhood interview videotapes 11 years before. Child Maltreatment, 2, 91-112.
Crews, F. (1995). The memory wars: Freud's legacy in dispute. New York: New York Review of Books.
Crews, F. (2003 (March 11)). The trauma trap [review of Remembering Trauma by R.J. McNally and Memory, Trauma Treatment, and the Law by D. Brown, A.W. Scheflin, & D.C. Hammond]. New York Review of Books, 51(4), 37-40.
Dawes, R. M. (1993). Prediction of the future versus an understanding of the past: a basic asymmetry. American Journal of Psychology, 106, 1-24.
Easterbrook, J. A. (1959). The effect of emotion on cue utilization and the organization of behavior. Psychological Review, 66, 183-201.
Eich, E., Macaulay, D., Lowewenstein, R. J., & Dihle, P. H. (1997). Memory, amnesia, and disociative identity disorder. Psychological Science, 8, 417-422.
Ellenberger, H. F. (1970). The discovery of the unconscious: The history and evolution of dynamic psychiatry. New York: Basic Books.
Erdelyi, M. H. (1990). Repression, reconstructio, and defense: History and integration of the psychoanalytic and experimental frameworks. In J. L. Singer (Ed.), Repression and dissociation: Implications for personality, psychopathology, and health (pp. 1-31). Chicago: University of Chicago Press.
Erdelyi, M. H., & Goldberg, B. (1979). Let's not sweep repression under the rug: Toward a cognitive psychology of repression. In J. F. Kihlstrom & F. J. Evans (Eds.), Functional disorders of memory (pp. 355-402). Hillsdale, N.J.: Erlbaum.
Fisher, C. (1945). Amnesic states in war neuroses: The psychogenesis of fugues. Psychoanalytic Quarterly, 3, 291-308.
Frederickson, R. (1992). Repressed memories: A journey to recovery from sexual abuse. New York: Simon & Schuster.
Freud, S. (1891/1953). On aphasia: A critical study. London: International Universities Press.
Freud, S. (1896). Futher remarks on the neuro-psychoses of defence. In J. Strachey (Ed.), The standard edition of the complete psychological works of Sigmund Freud (Vol. 3, pp. 159-185). London: Hogarth Press.
Freud, S. (1914/1957). The history of the psychoanalytic movement. In J. Strachey (Ed.), The standard edition of the complete psychological works of Sigmund Freud (Vol. 14, pp. 7-66). London: Hogarth Press.
Freud, S. (1915/1957). Repression. In J. Stravhey (Ed.), Thes tandrd edition of the complete psychological works of Sigmund Freud (Vol. 14, pp. 146-158). London: Hogarth Press.
Freyd, J. (1996). Betrayal trauma: The logic of forgetting childhood abuse. Cambridge, Ma.: Harvard University Press.
Ganaway, G. K. (1995). Hypnosis, childhood trauma, and dissociative identity disorder: Toward an integrative theory. International Journal of Clinical & Experimental Hypnosis, 43, 127-144.
Giglio, J. C. (1998). A comment on World War II repression. Professional Psychology: Research & practice, 29, 470.
Gleaves, D. H., smith, S. M., Butler, L. D., & Spiegel, D. (2004). False and recovered memories in the laboratory and clinic: A review of experimental and clinical evidence. Clinical Psychology: Science & Practice, 11, 3-28.
Goodman, G. S., Ghetti, S., Quas, J. A., Edelstein, R. S., Alexander, K. W., Redlich, A. D., Cordon, I. M., & Jones, D. P. H. (2003). A Prospective Study of Memory for Child Sexual Abuse: New Findings Relevant to the Repressed-Memory Controversy. Psychological Science, 14(2), 113-118.
Grinker, R. R., & Spiegel, J. P. (1943/1945). Men under stress. New York: McGraw-Hill.
Harvey, M. R., & Herman, J. L. (1994). Amnesia, partial amnesia, and delayed recall among adult survivors of childhood trauma. Consciousness & Cognition, 3, 374-387.
Herbart, J. F. (1816/1881). A textbook in psychology: An attempt to found the science of psychology on experience, metaphysics, and mathematics. New York: Appleton.
Herman, J. L. (1981). Father-daughter incest. Cambridge, Ma.: Harvard University Press.
Herman, J. S., & Schatzow, E. (1987). Recovery and verification of memories of childhood sexual trauma. Psychoanalytic Psychology, 4, 1-14.
Hilgard, E. R. (1977). Divided consciousness: Multiple controls in human thought and action. New York: Wiley-Interscience.
Holmes, D. S. (1974). Investigations of repression: Differential recall of material experimentally or naturally associated with ego threat. Psychological Bulletin, 81, 632-653.
Holmes, D. S. (1990). The evidence for repression: An examination of sixty years of research. In J. L. Singer (Ed.), Repression and dissociation: Implications for personality, psychopathology, and health (pp. 85-102). Chicago: University of Chicago Press.
Jacobs, W. J., Laurance, H. E., Thomas, K. G. F., Luzcak, S. E., & Nadel, L. (1996). On the veracity and variability of traumatic memory. Traumatology, 2(2).
James, W. (1890/1980). Principles of Psychology. Cambridge, Ma.: Harvard University Press.
Janet, P. (1889). [Psychological automatisms]. Paris: Alcan.
Janet, P. (1907). The major symptoms of hysteria. New York: Macmillan.
Kardiner, A., & Spiegel, H. (1941/1947). War, stress and neurotic illness (2d ed.). New York etc.: Hoeber.
Karon, B. P., & Widener, A. J. (1997). Repressed memories and World War II: Lest we forget! Profssional Psychology: Research & Practice, 28, 338-340.
Karon, B. P., & Widener, A. J. (1998). Repressed memories: The real story. Professional Psychology: Research & Practice, 29, 482-487.
Kendall-Tackett, K., & Marshall, R. (1998). Sexual victimization of children: Incest and child sexual abuse, Issues in intimate violence. (pp. 47-63). Thousand Oaks, CA, US: Sage Publications, Inc.
Kendall-Tackett, K. A., Williams, L. M., & Finkelhor, D. (1993). Impact of sexual abuse on children: A review and synthesis of recent empirical studies. Psychological Bulletin, 113(1), 164-180.
Kihlstrom, J. F. (1979). Hypnosis and psychopathology: Retrospect and prospect. Journal of Abnormal Psychology, 88(5), 459-473.
Kihlstrom, J. F. (1983). Instructed forgetting: Hypnotic and nonhypnotic. Journal of Experimental Psychology: General, 112(1), 73-79.
Kihlstrom, J. F. (1985). Posthypnotic amnesia and the dissociation of memory. Psychology of Learning and Motivation (G.H. Bower, Ed.), 19, 131-178.
Kihlstrom, J. F. (1992a). Dissociation and dissociations: A comment on consciousness and cognition. Consciousness & Cognition: An International Journal, 1(1), 47-53.
Kihlstrom, J. F. (1992b). Dissociative and conversion disorders, Cognitive science and clinical disorders. (pp. 247-270). San Diego, CA, USA: Academic Press, Inc.
Kihlstrom, J. F. (1994). One hundred years of hysteria. In S. J. Lynn & J. W. Rhue (Eds.), Dissociation: Clinical and theoretical perspectives. (pp. 365-394). New York, NY, USA: The Guilford Press.
Kihlstrom, J. F. (1996). The trauma-memory argument and recovered memory therapy. In K. Pezdek & W. P. Banks (Eds.), The recovered memory/false memory debate. (pp. 297-311). San Diego, CA, USA: Academic Press, Inc.
Kihlstrom, J. F. (1997). Suffering from reminiscences: Exhumed memory, implicit memory, and the return of the repressed. In M. A. Conway (Ed.), Recovered memories and false memories. (pp. 100-117). Oxford, England UK: Oxford University Press.
Kihlstrom, J. F. (1998). Exhumed memory, Truth in memory. (pp. 3-31). New York, NY, USA: The Guilford Press.
Kihlstrom, J. F. (2001). Dissociative disorders. In P. B. Sutker & H. E. Adams (Eds.), Comprehensive handbook of psychopathology (3rd ed., pp. 259-276). New York: Plenum.
Kihlstrom, J. F. (2002). No need for repression. Trends in Cognitive Sciences, 6, 502.
Kihlstrom, J. F. (2004a). Dissociative disorders. Annual Review of Clinical Psychology, 1, in press.
Kihlstrom, J. F. (2004b). An unbalanced balancing act: Blocked, recovered, and false memories in the laboratory and the clinic. Clinical Psychology: Science & Practice, 11, 34-41.
Kihlstrom, J. F. (2004, in press). Consciousness in hypnosis. In P. D. Zelazo & M. Moscovitch (Eds.), Cambridge Handbook of Consciousness (pp. in press). New York: Cambridge University Press.
Kihlstrom, J. F., Eich, E., Sandbrand, D., & Tobias, B. A. (2000). Emotion and memory: Implications for self-report, The science of self-report: Implications for research and practice. (pp. 81-99). Mahwah, NJ, US: Lawrence Erlbaum Associates, Inc., Publishers.
Kihlstrom, J. F., & Evans, F. J. (1979). Functional disorders of memory. Hillsdale, N.J.: Erlbaum.
Kihlstrom, J. F., & Evans, F. J. (1979). Memory retrieval processes in posthypnotic amnesia. In J. F. Kihlstrom & F. J. Evans (Eds.), Functional disorders of memory (pp. 179-218). Hillsdale, N.J.: Erlbaum.
Kihlstrom, J. F., & McGlynn, S. M. (1991). Experimental research in clinical psychology, The clinical psychology handbook (2nd ed.). (pp. 239-257). New York: Pergamon.
Kihlstrom, J. F., & Schacter, D. L. (2000). Functional amnesia. In F. Boller & J. Grafman (Eds.), Handbook of neuropsychology (2 ed., Vol. 2, pp. 409-427). Amsterdam: Elsevier.
Kihlstrom, J. F., Tataryn, D. J., & Hoyt, I. P. (1993). Dissociative disorders, Comprehensive handbook of psychopathology (2nd ed., pp. 203-234). New York, NY, USA: Plenum Press.
Kopelman, M. D. (2002). Psychogenic amnesia. In A. D. Baddeley & M. D. Kopelman & B. A. Wilson (Eds.), The handbook of memory disoders (2nd ed., pp. 451-471). Chichester, U.K.: Wiley.
Lange, A., DeBeurs, E., Dolan, C., Lchnit, T., Sjollema, S., & Hanewald, G. (1999). Long-term effects of childhood sexual abuse: Objective and subjective characteristics of the abuse and psychopathology in later life. Journal of Nervous & Mental Disease, 187, 150-158.
Levy, B. L., & Anderson, M. C. (2002). Inhibitory processes and the control of memory retrieval. Trends in Cognitive Sciences, 6, 299-305.
Lilienfeld, S. O., & Loftus, E. F. (1998). Repressed memories and World War II: Some cautionary notes. Professional Psychology: Research & Practice, 29, 471-475.
Loftus, E. F., Garry, M., & Feldman, J. (1994). Forgetting sexual trauma: What does it mean when 38% forget? Journal of Consulting & Clinical Psychology, 62, 1177-1181.
Loftus, E. F., & Guyer, M. J. (2002a). Who abused Jane Doe? Part 1. Skeptical Inquirer, 26(3), 24-32.
Loftus, E. F., & Guyer, M. J. (2002b). Who abused Jane Doe? Part 2. Skeptical Inquirer, 26(4), 37-40.
Lyon, L. S. (1985). Facilitating telephone number recall in a case of psychogenic amnesia. J Behav Exp, 16, 147-149.
MacKinnon, D. W., & Dukes, W. F. (1964). Repression. In L. Postman (Ed.), Psychology in the making (pp. 662-744). New York: Knopf.
Macmillan, M. (1997). Freud evaluated : the completed arc (1st MIT Press ed.). Cambridge, Mass.: MIT Press.
Markowitsch, H. J. (1999). Functional neuroimaging correlates of functional amnesia. MEMORY, 7(5-6), 561-583.
Markowitsch, H. J. (2000). Functional amnesia: the mnestic block syndrome. REVUE DE NEUROPSYCHOLOGIE, 10(1), 175-198.
Masson, J. M. (1984). The assault on truth : Freud's suppression of the seduction theory. New York: Farrar, Straus and Giroux.
McGaugh, J. L. (2004). The amygdala modulates the consolidation of memories of emotionally arousing experiences. Annual Review of Neuroscience, 27, 1-28.
McNally, R. J. (2003). Remembering trauma. Cambridge, Ma.: Harvard University Press.
Metcalfe, J., & Jacobs, W. J. (1996). A 'hot-system/cool-system" view of memory under stress. PTSD Research Quarterly, 7(2), 1-3.
Metcalfe, J., & Jacobs, W. J. (1998). Emotional memory: The effects of stress on "cool" and "hot" memory systems. In D. Medin (Ed.), The psychology of learning and motivation: Advances in theory and research (Vol. 38, pp. 187-222). San Diego: Academic.
Metcalfe, J., & Jacobs, W. J. (2000). Can 'hot' human emotions be captured by "cool" mathematical models? In E. Tulving (Ed.), Memory, consciousness, and the brain: The Tallinn Conference (pp. 228-242). Philadelphia: Psychology Press.
Mineka, S., & Kihlstrom, J. F. (1978). Unpredictable and uncontrollable events: A new perspective on experimental neurosis. Journal of Abnormal Psychology, 87(2), 256-271.
Nadel, L., & Jacobs, W. J. (1998). Traumatic memory is special. Current Directions in Psychological Science, 7(5), 154-157.
O'Brien, J. T. (1997). The 'glucocorticoid cascade' hypothesis in man: Prolonged stress may cause permanent brain damage. British Journal of Psychiatry, 170, 199-201.
Pendergrast, M. (1996). Victims of memory : sex abuse accusations and shattered lives (2nd, updated and expanded ed.). Hinesburg, Vt.: Upper Access.
Pendergrast, M. (1998). Response to Karon and Widener (1997). Professional Psychology: Research & Practice, 29, 479-481.
Piper, A. (1998). Repressed memories from World War II: Nothing to forget. Examining Karon and Widener's (997) claim to have discovered evidence for repression. Professional Psychology: Research & Practice, 29, 476-478.
Piper, A. (1999). A skeptic considers, then responds to Cheit. Ethics & Behavior, 9, 277-293.
Piper, A., Pope, H. G., & Borowiecki, B. S. (2000). Custer's last stand: Brown, Schefflin, and Whtfield's latest attempt to salvage "dissociative amnesia". Journal of Psychiatry & Law, 28, 149-213.
Pope, H. G., & Hudson, J. I. (1995). Can individuals "repress" memories of childhood sexual abuse? An examination of the evidence. Psychiatric Annals, 25(12), 715-719.
Pope, H. G., & Hudson, J. I. (1995). Does childhood sexual abuse cause adult psychiatric disorders? Essentials of methodology. Journal of Psychiatry & Law(Fall), 363-381.
Pope, H. G., Jr., Hudson, J. I., Bodkin, J. A., & Oliva, P. (1998). Questionable validity of "dissociative amnesia" in trauma victims: Evidence from prospective studies. British Journal of Psychiatry, 172, 210-215.
Pope, H. G., Oliva, P. S., & Hudson, J. I. (2000). Repressed memories: B. Scientific status. In D. L. Faigman & D. H. Kaye & M. J. Saks & J. Sanders (Eds.), Modern scientific evidence: The law and science of expert testimony (Vol. 1, 2000 Pocket Part, pp. 154-195). St. Paul, Mn.: West Publisher.
Rapaport, D. (1942). Emotions and memory. Baltimore, Md.: Williams & wilkins.
Rind, B. (2003). An elaboration on causation and positive cases in child sexual abuse. Clinical Psychology: Science & Practice, 10, 352-357.
Rind, B., Tromovich, P., & Bauserman, R. (1998). A meta-analytic examination of assumed properties of child sexual abuse using college samples. Psychological Bulletin, 124, 22-53.
Ross, C. A. (1986). Multiple personality disorder: Diagnosis, clinical features, and treatment. New York: Wiley.
Sbraga, T. P., & O'Donohue, W. (2003). Post hoc reasoning in possible cases of child sexual abuse: Symptoms of inconclusive origins. Clinical Psychology: Science & Practice, 10, 320-334.
Scarf, M. (2004). Secrets, lies, betrayals: The body/mind connection. New York: Random House.
Schacter, D. L. (1987). Implicit memory: History and current status. Journal of Experimental Psychology: Learning, Memory, and Cognition, 13, 501-518.
Schacter, D. L. (2001). Suppression of unwanted memories: Repression revisited? Lancet, 357, 1724-1725.
Scheflin, A. W., & Brown, D. (1996). Repressed memory or dissociative amnesia: What the science says. Journal of Psychiatry & Law, 24(2), 143-188.
Schooler, J. W. (2001). Discovering memories of abuse in the light of meta-awareness. Journal of Aggression, Malteratment & Trauma, 4, 105-136.
Schreiber, F. R. (1973). Sybil: The true story of a woman possessed by 16 separate personalites. Chicago: Regnery.
Sears, R. R. (1936). Functional abnormalities of memory with special reference to amnesia. Psychological Bulletin, 33, 229-274.
Shobe, K. K., & Kihlstrom, J. F. (1997). Is traumatic memory special? Current Directions in Psychological Science, 6(3), 70-74.
Singer, J. L. (Ed.). (1990). Repression and dissociation: Implications for personality theory, psychopathology, and health. Chicago: University of Chicago Press.
Swets, J. A., Dawes, R. M., & Monahan, J. (2000). Psychological science can improve diagnosic decisions. Psychological Science in the Public Interest, 1(1), 1-26.
Terr, L. (1994). Unchained memories: True stories of traumatic memories, lost and found. New York: Basic Books.
Thigpen, C. H., & Cleckley, H. (1954). A case of multiple personality. Journal of Abnormal & Social Psychology, 135-151.
Thigpen, C. H., & Cleckley, H. (1984). On the incidence of multiple personality disorder. International Journal of Clinical & Experimental Hypnosis, 32, 63-66.
Thigpen, C. H., & Cleckley, H. M. (1957). The three faces of Eve. New York: Popular Library.
Thomas, K. G. F., Laurance, H. E., Jacobs, W. J., & Nadel, L. (1995). Traumatic memory and its recovery: Formulating hypotheses and critical experiments. Traumatology, 1(2).
van der Kolk, B. A. (1994). The body keeps the score: Memory and the evolving psychobiology of posttraumatic stress. Harvard Review of Psychiatry, 1, 253-265.
van der Kolk, B. A., & Fisler, R. (1995). Dissociation and the fragmentary nature of traumatic memories: Overview and exploratory study. Journal of Traumatic Stress, 8(4), 505-525.
van der Kolk, B. A., & Fisler, R. E. (1993). The biologic basis of posttraumatic stress. Family Violence & Abusive Relationships, 20, 417-432.
Walker, L. E. (1994). Abused women and survivor therapy: A practical guide for the psychotherapist. Washington, D.C.: American Psychological Association.
Wegner, D. M. (1989). White bears and other unwanted thoughts: Suppression, obsession, and the psychology of mental control. New York: Penguin.
Wegner, D. M., Schneider, D. J., Carter, S. R., & White, T. L. (1987). Paradoxical effects of thought suppression. Journal of Personality and Social Psychology, 53, 5-13.
Widom, C. S., & Morris, S. (1997). Accuracy of adult recollections of childhood victimization. Part 2: Childhood sexual abuse. Psychological Assessment, 9, 34-46.
Williams, L. M. (1994). Recall of childhood trauma: A prospective study of women's memories of child sexual abuse. Journal of Consulting & Clinical Psychology, 62, 1167-1178.
Yerkes, R. M., & Dodson, J. D. (1908). The relation of strength of stimulus to rapidity of habit-formation. Journal of Comparative & Neurological Psychology, 18, 459-482.
Zeller, A. (1950). An experimental analogue of repression: I. Historical summary. Psychological Bulletin, 47, 39-51.
This page last modified 04/08/10 02:58:52 PM.