In introducing the scientific study of
mind and behavior, we have focused primarily on adaptive
behavior, and the normal mental processes that underlie it.
There have been occasional references to cases of brain
insult, injury, and disease, for the light they shed on normal
mental life. Now we wish to examine mental illness in its own
right:
abnormal and maladaptive behavior;
the disordered mental processes that underlie it;
and interventions that treat and prevent mental illness.
The term psychopathology is,
obviously, derived from two Greek roots:
psycho, from the Greek psyche, soul,
referring to the mind;
pathology, from the Greek pathos,
suffering, referring to disease or illness.
The term makes it clear that mental
illness is analogous to physical illness. Just as physical
illness involves abnormalities of bodily structure (anatomy)
and function (physiology), so mental illness involves
abnormalities of mental structure and function --
abnormalities of cognition, emotion, and motivation -- that
result in abnormal, deviant behavior.
Defining Psychopathology
It has not proved easy to define
psychopathology in the abstract.
By analogy with the concept of
pathology in medicine, psychopathology may be defined as
abnormalities in mental structures, processes, and states that
give rise to abnormal, deviant behavior. But the concept of abnormality
implies an opposite construct of normality, from which
abnormality deviates. So what do we mean by normality?
Normal mental and behavioral
functioning is characterized by:
Accurate and Efficient Cognition: Normal people
generally see the world the way it is, remember things the
way they happened, think clearly, and communicate
comprehensibly. And beyond cognition, they tend to have
feelings and desires that are appropriate to the
situation.
Self-Awareness: Normal people generally are aware
of their thoughts, feelings, and desires, and of their
behavior and its impact on other people.
Self-Control Normal people generally are able to
control their impulses and emotions, and to delay
gratification.
Self-Esteem: Normal people generally think
reasonably well of themselves.
Social Relations Based on Affection: Normal
people generally treat others with respect, and not like
objects.
Productivity and Creativity: Normal people are
generally productive at work, at play, and in their family
lives; and although most of us can't become great artists,
we are nevertheless able to create things on our own.
(Note: I am pretty certain that I
derived this list of features of normality from an early
edition of a textbook in abnormal psychology written either by
Richard Bootzin, or one by Gerald Davison and John Neale, but
I can no longer identify the source precisely.)
But having defined a sort of prototype
for "normality", what do we mean by deviance?
Deviations from normality can be
defined in various ways:
Deviance from Statistical Norms: By statistical
convention, a score is "abnormal" if it lies more than 2
standard deviations above or below the population mean.
This frequency criterion is certainly
objective, but it has some problems attached to it --
not the least of which is the problem of estimating
population means for all the various mental
characteristics on which people might deviate.
There is also the problem of what to do about positive
deviations. An IQ less than 70 is more than 2 standard
deviations away from the mean IQ of 100, and (if other
factors are also present) can lead an individual to be
classified as intellectually disabled (what used to be
known as "mental retardation"). But an IQ of more than
130 is also more than 2 standard deviations away from
the mean, and can lead an individual to be classified as
a "genius". But while intellectual disability is a form
of mental illness, we usually don't think of genius that
way. A further problem is that even negative deviations
are not necessarily signs of mental abnormality. For
example, a person who is more than 2 standard deviations
below the mean on Extraversion might be merely
shy.
Deviance from Social Norms: Every group,
organization, and society imposes certain expectations and
demands on its members, and some people simply don't do
what they are supposed to do. Given that human experience,
thought, and action takes place in an expressly social
context, this compliance criterion may well be
useful for evaluating which deviations we should pay
attention to, but it also has its problems.
Norms vary across societies. In the former Soviet
Union, political dissidents could be classified as
mentally ill, and confined to mental hospitals, simply
for disagreeing with their government.
Norms also vary across epochs within societies. When I
began my graduate studies, in 1970, homosexuality listed
in the official Diagnostic and Statistical Manual of
Mental Disorders. Then, about 1973, the American
Psychiatric Association took a vote and decided that it
wouldn't call homosexuality a mental illness any
longer.
One may agree with the vote (as I do), but the
essentially political process by which the status of
homosexuality was changed should give us pause. If we
are looking for an objective standard by which to
evaluate deviance, we want one that is constant across
groups. The length of a foot or a yard doesn't vary
from Denmark to Ghana -- why should the criteria for
mental disorders be any different?
Personal Distress: mental illness is usually
manifested in symptoms that create problems for the
patient, and cause considerable concern. This subjective
criterion may be important in leading the patient to
seek the help of a professional, but it too has a couple
of problems.
People's self-perceptions are not always accurate.
Some people believe they are ill when they are not; but
more important in the present context, some mentally ill
people do not believe that they are mentally ill, and
resist diagnosis and treatment. This is a particular
problem in schizophrenia and the personality disorders.
Even when people's self-perceptions are accurate, we
would not want to substitute self-diagnosis for an
objective assessment by a trained professional. We don't
let patients self-diagnose cancer and heart disease --
why should we allow them to self-diagnose depression and
anxiety disorder?
Maladaptiveness: Mental illness often leads
people to engage in behaviors that are harmful to
themselves and others. For example, people with depression
may be at elevated risk for suicide. People with
antisocial personality disorder, by definition, engage in
antisocial behaviors. Normal mental function is by
definition adaptive, because the purpose of the mind is to
aid the organism's adaptation to its environment, so a harmfulness
criterion is helpful in diagnosing mental illness. On the
other hand:
Not all maladaptive behavior is a sign of mental
illness. Criminal behavior is maladaptive, harmful to
the people against whom the crime is perpetrated, and
harmful to the criminal when he or she is caught and
punished. But we do not label all criminal behavior as
the product of mental illness. In fact, the insanity
defense is attempted in only a very small minority of
criminal cases, and it is successful in only a very
small minority of these.
The Insanity Defense
In 1981, John Hinckley attempted to assassinate
President Ronald Reagan: one of his gunshots
actually hit Reagan, and others seriously injured
James Brady, Reagan's press secretary, a Secret
Service agent, and a District of Columbia
policeman. Hinckley's motive was a desire to
impress Jodie Foster, an actress, with whom he was
infatuated. At his trial, in 1982, a jury
found him not guilty by reason of insanity.
More than 30 years later, he remains confined to St.
Elizabeth's Hospital, a federal facility in
Washington D.C.
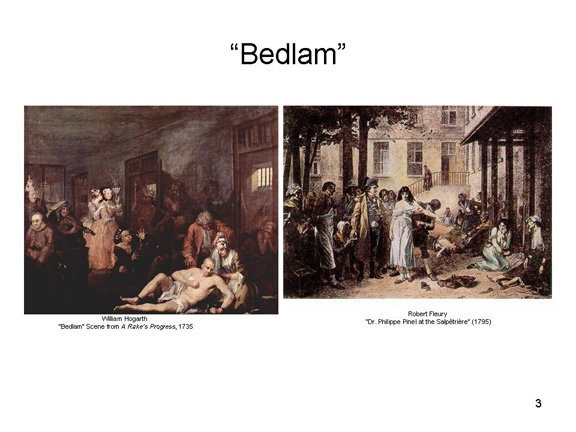
Up until the late 18th century, the mentally ill
were treated little differently than
criminals. It wasn't until after the French
Revolution that Jean-Etienne Dominique Esquirol
formally distinguished between insanity, mental
deficiency, and criminality, and his protege
Phillippe Pinel "freed the insane from their
chains". As medicine developed further,
however, psychiatrists began to understand that, in
certain instances, criminal behavior could be a
product of insanity. If that were the case,
then the "criminal" could not be held morally and
legally responsible for his or her criminal acts.
At lest since the 17th century, English common law
has required that a criminal act (actus rea,
or "guilty act") be accompanied by criminal intent (mens
rea, or "guilty mind". There is no
criminal liability for injuries committed
involuntarily (e.g., because of a reflex, or while
sleepwalking).
The formal insanity defense has its beginnings in
1843, when Daniel McNaughton tried to kill Robert
Peel, the British prime minister (he shot and killed
his secretary instead). At his trial,
McNaughten testified that he believed that the
British government was plotting against him, and he
was acquitted of murder. The McNaughton
Rule requires that a criminal defendant (1)
not know what he was doing at the time or (2) not
know that his actions were wrong (because of his
delusional belief, McNaughton thought he was
defending himself).
In the United States, the next advance in the
insanity defense was The Durham Rule or
"product test" adopted in 1954, which states that
"... an accused is not criminally responsible if his
unlawful act was the product of mental disease or
defect". This "product test" was overturned in
1972, largely because its ambiguous reference to
"mental disease or defect" places undue emphasis on
subjective judgments by psychiatrists, and can
easily lead to a "battle of the experts".
Many states now adopt a version of guidelines set
out by the American Law Institute in 1962, which
allows the insanity defense if, by virtue of mental
illness, the defendant (1) lacks the ability to
understand the meaning of their act or (2) cannot
control their impulses. This is sometimes
known as the "irresistible impulse test".
Other states allow for a compromise verdict of
"guilty but mentally ill", resulting in commitment
to a mental institution for treatment, rather than
incarceration in a prison for punishment.
In whatever form, the insanity defense requires
both that the defendant meet the criteria for some
psychiatric diagnosis and that his
ostensibly criminal act be attributed to his mental
illness.
Hinckley clearly met this criterion, but the
insanity defense is rarely successful. It has
been estimated that it is invoked in only about 1%
of criminal trials, and it succeeds in fewer than
25% of those cases. And while commitment to a
mental hospital is arguably better than
incarceration in a prison, there is a definite
downside. Prison terms lapse, and prisoners
can be released or paroled. But commitment to
a mental hospital can be forever -- until the
relevant medical authorities can persuade a judge
that their patient's illness has been
resolved.
Lynette "Squeaky" Fromme, who attempted to
assassinate President Gerald Ford in 1975, was
sentenced to life in prison and paroled in 2009.
Hinckley remained in St. Elizabeth's until 2016,
when he was, effectively, paroled to house
arrest. He now lives with his aged mother,
and cannot travel more than 30 miles from her
house without supervision.
The links between psychology and the law go far
beyond the insanity defense. Cognitive
psychologists have studied the problems created by
the unreliability of eyewitness testimony, and
social psychologists have studied how juries, and
individual jurors, arrive at verdicts of guilty or
not guilty.
For a recent survey of the relations between
neuroscience and the legal system, see "Neuroscience
and the Law: Don't Rush In" by Jed Rakoff, a
prominent Federal District Court Judge (New
York Review of Books, 05/12/2016).
Each of these definitions has certain
assets and liabilities. Taken together, these two lists of
definitions -- of normality and of deviance -- comprise a kind
of "prototype" of the "typical" case of mental illness. Not
every mentally ill person will lack all the criteria of
normality, or display all the criteria of deviance. But most
mentally ill people will display some or most of them, so that
the mentally ill are related to each other by a principle of
family resemblance.
Syndromes of Mental Illness
In actual practice, mental illnesses
are not identified by abstract conceptual definitions of
mental abnormality and deviance, but rather in terms of
various syndromes characterized by particular signs and
symptoms.
The Diagnostic Nosology
I
identify nine (9) major categories of mental illness.
Warning: these groupings differ somewhat from such "official"
classifications as the Diagnostic and Statistical Manual
of the American Psychiatric Association, but the overlaps are
clear.
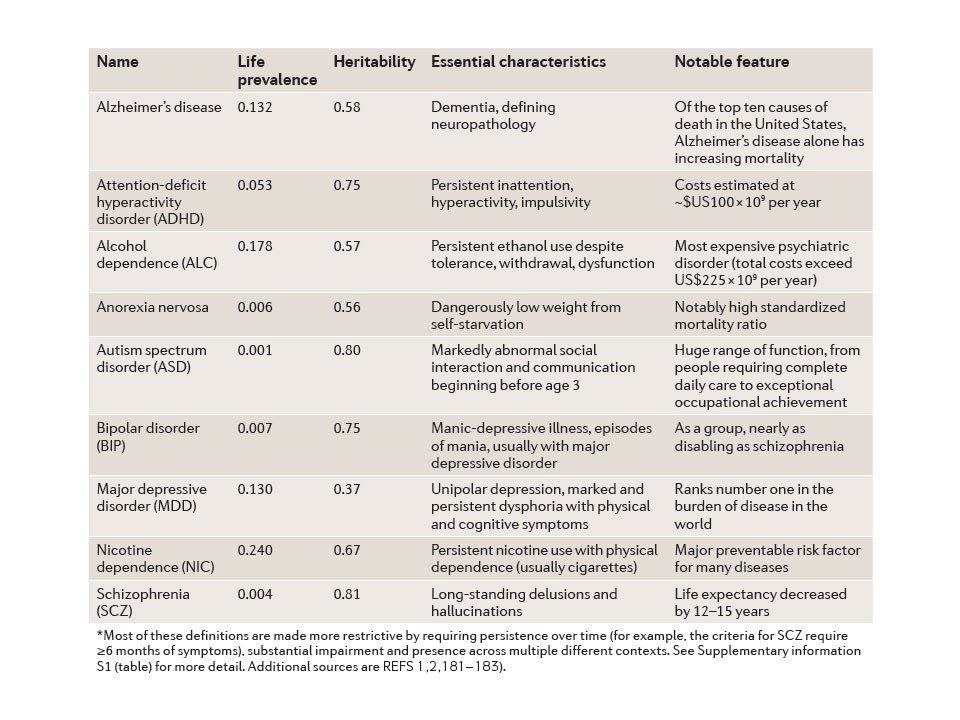
1. Organic Brain Syndromes,in
which there are gross impairments in mental function resulting
from known insult, injury, or disease in the central nervous
system.
Alzheimer's disease is a clear example: here the
patient suffers memory loss and other aspects of dementia
resulting from plaques and tangles in cortical tissue.
Other examples are the amnesic syndrome (such as
Patient H.M.) associated with damage to the hippocampus
and related areas,
and the various forms of aphasia associated with
damage to Broca's and Wernicke's areas.
2. Developmental
Disorders,in which there is an abnormal pace of
development in one or more mental functions since birth.
The
classic example is intellectual disability, in
which the individual shows subnormal levels of mental
function (as indexed by an IQ less than 70), in degrees
ranging from mild to profound, accompanied by an inability
to meet the demands of his or her environment.
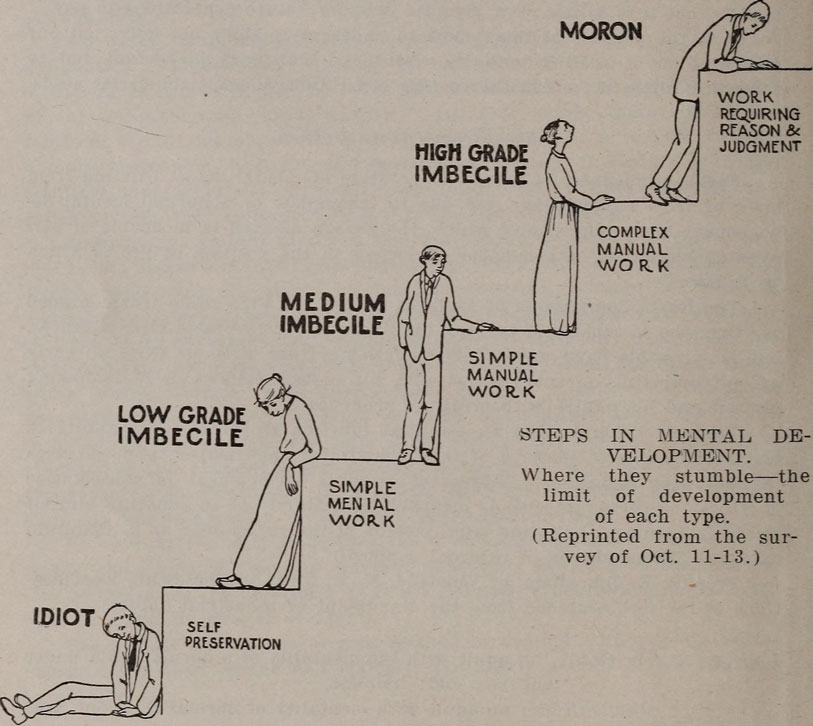
Henry H. Goddard, an early authority on intelligence,
classified what was then known as "mental retardation"
into three subcategories -- moron, idiot,
and imbecile -- based strictly on IQ test scores
(Illustration above right from the state government
report on Mental Defectives in Virginia
(1915).
More recent practice has abandoned these offensive
terms, but more importantly assess intellectual
disability not just in terms of test scores, but also in
terms of the individual's ability to cope with
environmental demands. If people with low IQs can
get along effectively in their environment, there is no
reason to classify them as intellectually disabled.
DSM-5 assesses the severity of intellectual
disability from mild t profound, taking account of the
individual's ability to adapt in the social and
practical as well as the purely intellectual domains.
Similarly, the American Association for Intellectual
and Developmental Disabilities (formerly the American
Association for Mental Retardation) takes account of
how much environmental support the individual needs,
from intermittent to pervasive.
Another example is autism, a disorder
characterized by a severe inability to relate to, and
communicate with, other people. Autism is now often
referred to as autism spectrum disorder, an
umbrella term that covers conditions like Asperger's
syndrome as well.
Traditionally, classical autism was characterized by
three criteria: impairment in social interaction;
impairment in social communication (language); and
restricted, repetitive and stereotyped patterns of
behavior, interests, and activities. Asperger's syndrome
was used for patients who displayed impairments in
social interaction but not impairments in
language. The 5th edition of the Diagnostic
and Statistical Manual of Mental Disorders (DSM-5)
collapses social interaction and social communication
into a single criterion, and has been very
controversial.
Attention deficit hyperactivity disorder (ADHD),
a relatively new syndrome, is typically diagnosed in
children. Originally, it was thought that children would
"outgrow" ADHD with time, but in fact many children with
ADHD grow up to be adults with ADHD, and the syndrome is
now diagnosed and treated in adults as well.
Originally, the syndrome was called "hyperactivity" or
"hyperkinetic disorder".
The syndrome entered the diagnostic nomenclature as
Minimal Brain Dysfunction (MBD) in DSM-II (1968)
-- "minimal" because there was no physical evidence of
any brain damage.
Following an argument by Virginia Douglas (1972), a
Canadian psychologist, that the basic problem in
"hyperkinesis" was insufficient attention, the syndrome
was renamed at Attention Deficit Disorder (ADD) in DSM-III
(1980)
In DSM-IIIR (1987), the diagnosis was expanded
to Attention deficit Hyperactivity Disorder (ADHD).
Intellectual Disability and the Death Penalty
In 2002, in the case of Daryl R. Atkins (Atkins
v. Virginia), a convicted murderer with an IQ of 59,
the United States Supreme Court prohibited the execution of
intellectually disabled prisoners. However, the Court did
not provide guidelines for determining who is intellectually
disabled. Instead, the Court left it up to individual
states to determine the standards by which intellectual
disability is diagnosed -- provided that they are "informed
by the medical community's diagnostic framework" (Hall v.
Florida, 2014). Accordingly, some two years
later, Atkins still faced the death penalty ("New Challenge
for Courts: How to Define Retardation" by Adam Liptak,New
York Times, 03/14/04).
One problem is the way intellectual disability
is defined in the psychiatric nosology: subnormal IQ plus
a demonstrated inability to meet environmental demands. The
reasonable approach would be to adopt the standards set by
the DSM or the similar standards promoted by the
AAIDD. But even so, low test scores can be faked, and
judgments of adaptiveness are inherently subjective. These
problems are confounded by the theory, promoted by some
prosecutors and other proponents of the death penalty, that
certain murders (such as the one Atkins was convicted of
committing) require highly sophisticated planning, and
therefore are beyond the capacity of the intellectually
disabled. Even "low IQ" is problematic: an IQ below 70
is two standard deviations below the mean, but all such
measurements are somewhat unreliable. Should someone
with an IQ of 71 be put to death just because he or she
A 2004 ruling by the Texas Court of Criminal
Appeals (ex parte Brisno) essentially adopted
Virginia's reasoning, effectively ruling intellectual
disability out in cases where a crime entailed "forethought,
planning, and complex execution of purpose". The ruling
poses an interesting "Catch-22": a defendant's crime can be
used to impeach the claim that he or she is intellectually
disabled! As it happens, the standards in Texas,
whose public officials have an inordinate fondness for the
death penalty, are not only outmoded, they include various
stereotypes about the intellectually disabled, which have no
scientific basis. In fact, Judge Cochran, writing for
the Texas CCA, referred to Lennie Small, the "retarded"
character in John Steinbeck's novel, Of Mice and Men
(1937) -- she actually talked of "the Lennie standard"
("Supreme Court to Consider Legal Standard Drawn from 'Of
Mice and Men'" by Adam Liptak, New York Times,
08/22/2016). The effect of these standards, if that is
what they are, is to severely limit those who would qualify
as intellectually disabled.
Moore v Texas, a case brought before
the Supreme Court in 2016, challenges the Texas standards in
a case of a man convicted in 1980 of murder in the
course of a robbery. Moore's death sentence was
overturned by a lower court, which used modern medical
standards to determine that he was intellectually disabled,
and thus could not be executed. The Texas CCA reversed
that decision, expressly criticizing the lower court judge
for applying contemporary scientific standards, instead of
the ones set out in earlier decisions by the CCA.
These standards, in the CCA's view, more closely reflect the
beliefs about intellectual disability held by ordinary
Texans -- scientific evidence and medical standards be
damned. In 2017, the Court overturned the Texas
decision by 5-3, ruling that the Texas court relied too
heavily on IQ scores -- not to mention outmoded stereotypes
about the intellectually disabled. The Court advanced
a new three-point standard for identifying the
intellectually disabled:
"Sub average intellectual functioning", meaning IQ
scores lower than "approximately 70".
Lack of fundamental social and practical skills.
Presence of both of these conditions before the age of
18.
Three justices dissented, on the grounds that Moore's two
"reliable" IQ scores were both over 70 -- high enough to
permit his execution.
3. Psychoses,
in which there are gross impairments in reality testing.
Psychoses are often labeled as "functional", meaning that they
have no organic cause. However, these disorders are almost
certainly "organic" in nature, and as their underlying brain
pathology becomes known they may well be shifted to the
category of organic brain syndromes.
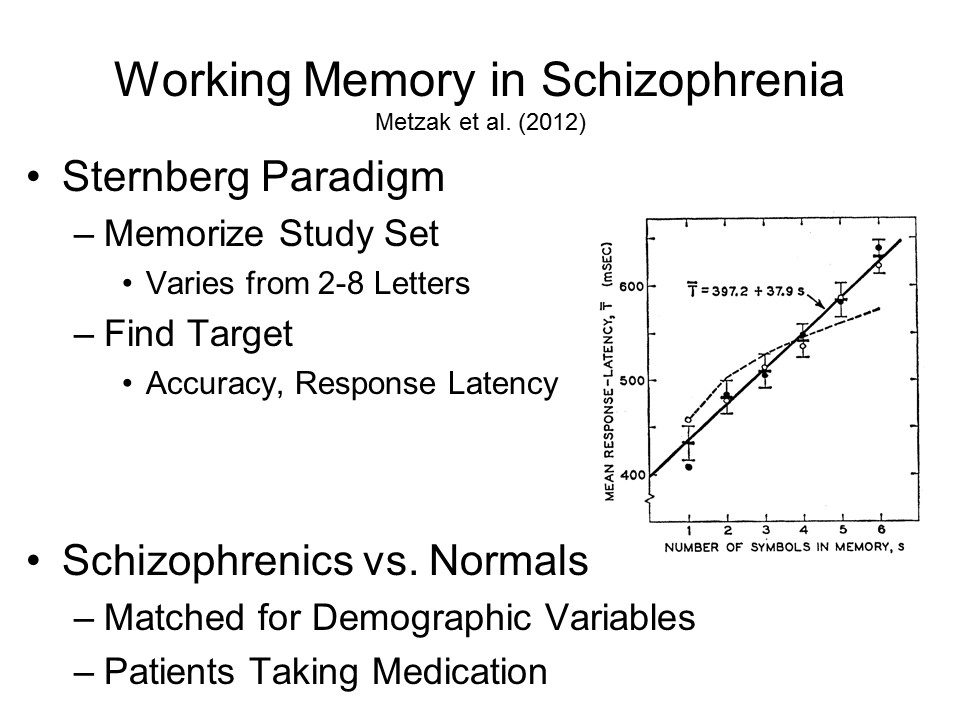
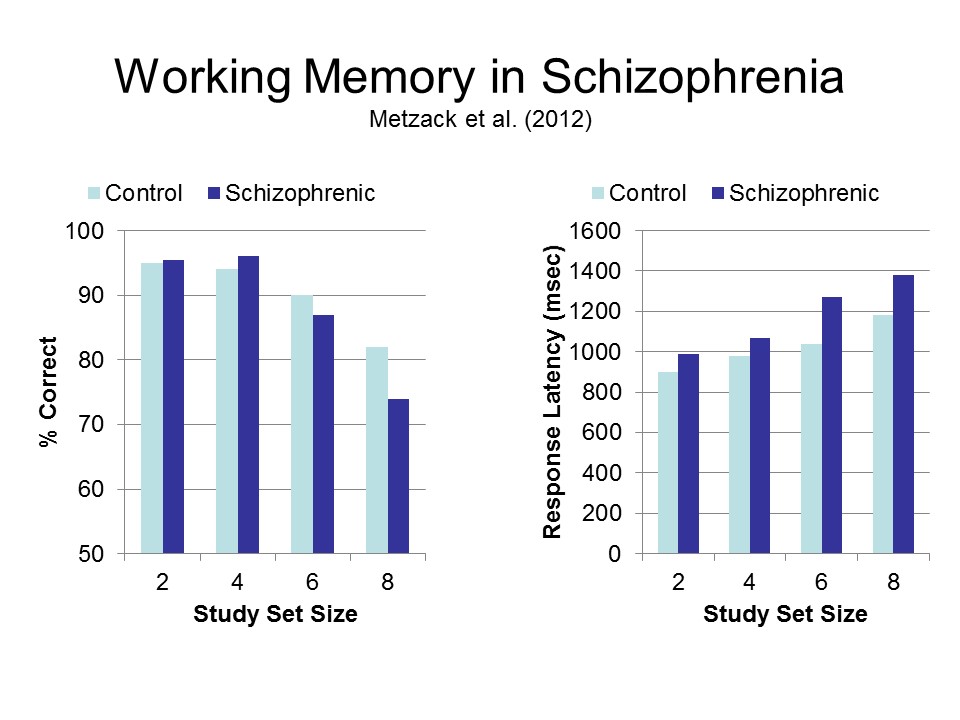
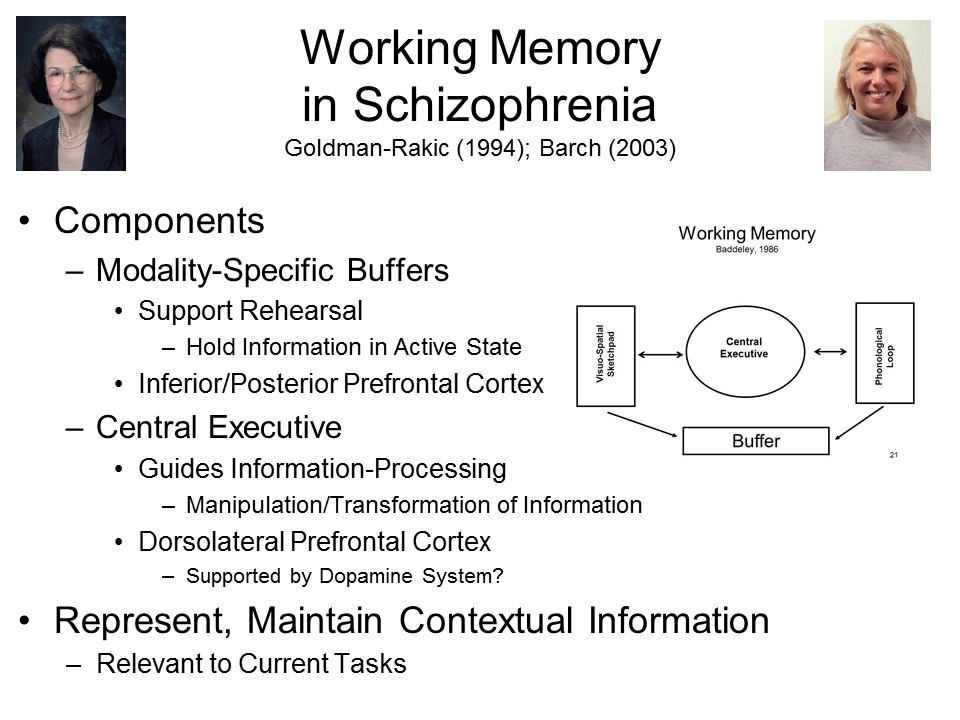
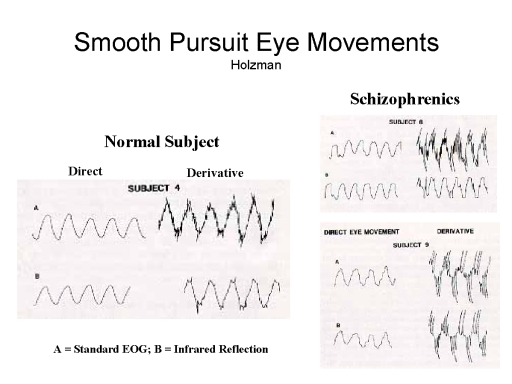
Schizophrenia, characterized by disordered
language and thought processes.
Very early medical texts, going back to the Egyptian Book
of Hearts and the Chinese Yellow emperor's
Classic of Internal Medicine describe illnesses
resembling modern-day schizophrenia.
In 1809, Phillippe Pinel described a "premature
dementia" in young patient
In 1896, Emile Kraepelin renamed the disorder dementia
praecox, or "early dementia", distinguishing the
disorder from the "senile dementia" associated with
aging.
The term schizophrenia was introduced by Eugen
Bleuler (1911), who distinguished among five subtypes:
Simple
Hebephrenic (childlike)
Catatonic (immobile)
Paranoid (delusional)
Chronic Undifferentiated
Schneider (1959) characterized schizophrenia in terms
of a set of "first-rank" symptoms:
Auditory hallucinations, particularly voices
speaking to the patient (arguing or giving
instructions.) or about the patient (commenting on the
patient's actions).
Schneider considered other hallucinations to be
"second-rank" symptoms.
Experience of one's mind or body being controlled.
Thought disorder:
That one's thoughts are being heard aloud.
Thought withdrawal/
Thought insertion.
Thought broadcasting.
Delusional perceptions, in which an actual stimulus
event (not a hallucination) is given a bizarre
interpretation.
A variety of affective disorders, primarily
affecting emotional functioning (as their name implies),
including
major depressive disorder (also known as unipolar
depression),
bipolar disorder (formerly known as manic-depressive
illness,
and pure mania.
4. Neuroses, a set of
syndromes that share primary symptoms of anxiety in common.
These are also "functional" in nature, but in contrast to the
psychoses there is less question of organic involvement;
rather, they are commonly attributed to the patient's
experiential history of social learning.
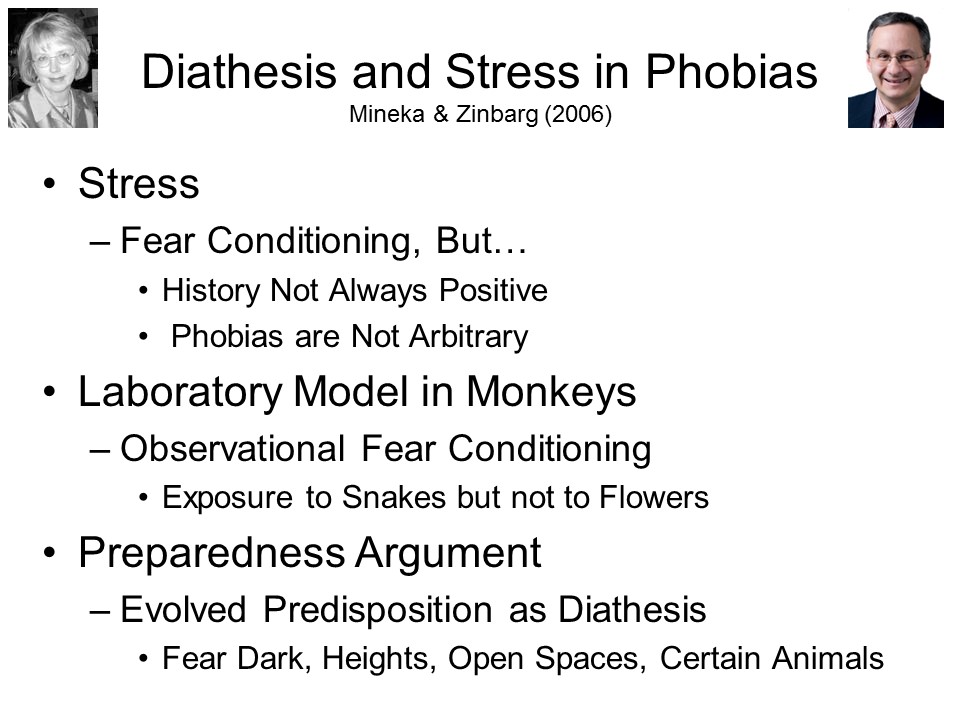
A variety of phobic disorders, entailing
excessive, unwarranted, and irrational fears of specific
objects or situations, such as snakes and spiders,
heights, open spaces, or public places.
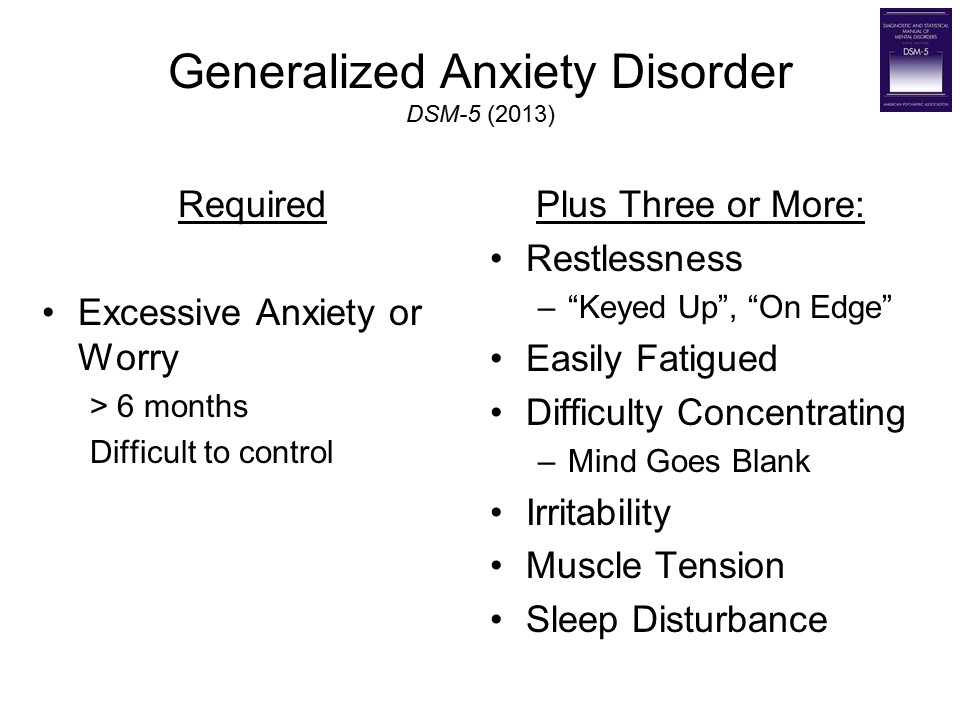
In contrast, anxiety disorder is characterized by
a free-floating state of apprehension and worry,
unattached to any object.
Sudden, unexpected waves of anxiety are characteristic
of panic disorder.
For an excellent personal account of anxiety disorder,
see My Age of Anxiety: Fear, Hope, Dread, and the
Search for Peace of Mind by Scott Stossel.
Obsessive-compulsive disorder (OCD) is
characterized by recurring, unwanted ruminations about
certain events (past or future), often accompanied by
overt behaviors intended to reduce the impact of these
events, or the likelihood that they will occur.
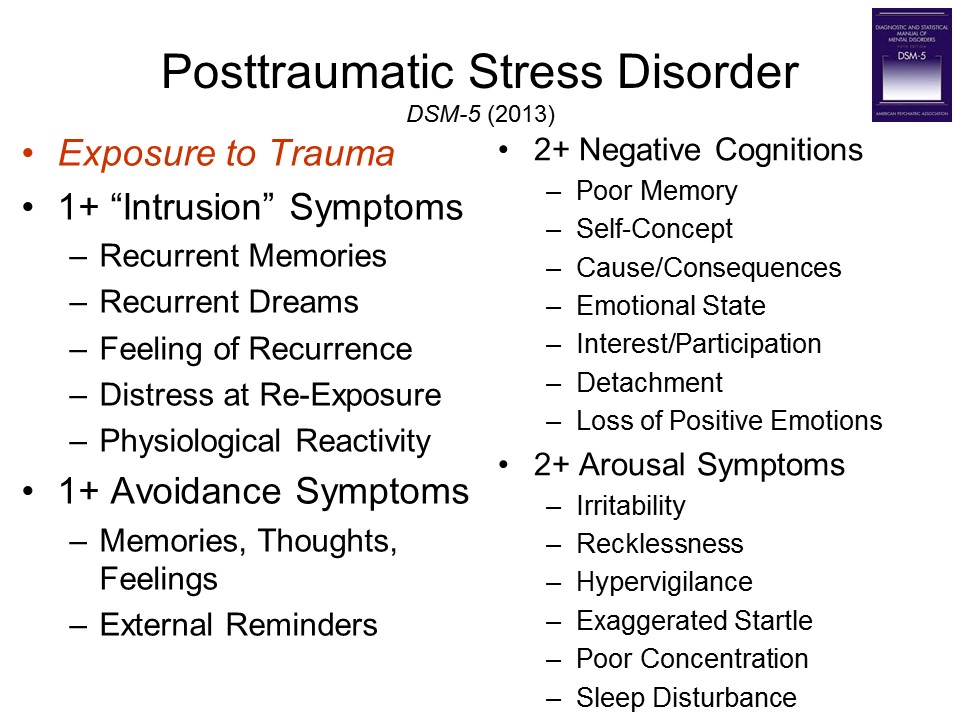
As its name implies, post-traumatic stress disorder
occurs in some individuals who have been exposed to high
levels of stress, such as soldiers on a battlefield,
victims of sexual assault and other violent crimes, and
victims of natural disasters such as earthquakes and
hurricanes (for a review, see Rosen & Lilienfeld,
2008).
The syndrome was first recognized in World War I: the
term "shell shock" first appeared in the Lancet,
a British medical journal, in 1915. As its name
implies, it was originally attributed to a kind of
concussion, caused by artillery shells exploding near
the soldier, and the resulting "commotion" in the
brain. Affected soldiers received a war ribbon and
a disability pension. However, cases began to be
diagnosed in soldiers who had been nowhere near
exploding ordnance, leading psychiatrists to shift their
thinking. Now, "shell shock" was called "war
neurosis", and viewed as reflecting a "nervous
breakdown" or neurasthenia -- emotional
shock, if you will, rather than concussion or
"commotional" shock. Instead of recovering from
their putative brain injuries in hospitals, they were
now sent to convalesce in mental hospitals. (See
"the Shock of War" by Caroline Alexander, Smithsonian,
September 2010).
War neurosis was diagnosed in World War II, as well,
where it was the subject of an important documentary
film, Let There Be Light, directed by by John
Huston -- a film that the War Department censored,
worried that the public would balk at learning about
the psychological damage wreaked by
warfare.
And, in retrospect, war neurosis occurred before
World War I, as well.
In the Civil War, is was known as "irritable
heart", or Da Costa's Syndrome" (see "PTSD: The
Civil War's Hidden Legacy" by Tony Horwitz, Smithsonian
Magazine, 01/2015).
War neurosis, redefined as PTSD, surfaced with a
vengeance during the Vietnam War (it was originally
called "post-Vietnam syndrome"), and again in the
post-9/11 wars in Afghanistan and Iraq (as well as en
epidemic of concussive head injuries caused by
improvised explosive devices, or IEDs).
At roughly the same time, mental health professions
began to appreciate the effects of trauma off the
battlefield, especially in victims of sexual assault
and of childhood sexual and physical abuse. PTSD
formally entered the diagnostic nosology with the
third edition of the Diagnostic and Statistical
Manual for Mental Disorders (DSM-III), in
1980 (Scott, 1990).
One positive result of the wars in Iraq and
Afghanistan is that soldiers suffering from PTSD can
now receive disability benefits -- even if they did
not directly experience the trauma in question.
Just being in the vicinity, apparently, was
traumatic enough. This policy change, however,
only served to increase the controversy over the
diagnosis. Contributing to the debate was the
proposal that veterans with PTSD receive a medal,
analogous to the Purple Heart, to recognize their war
injuries -- mental injuries, rather than physical
injuries, but injuries just the same.
Usually we think of PTSD we think about victims of
violent crime, or war, or natural disaster. And
that's how psychiatrists usually think about it,
too. The Diagnostic and Statistical Manual of
Mental Disorders (DSM) defines stress as
experiencing, or witnessing, "actual or threatened death
or serious injury, or a threat to the physical integrity
of self or others". But as we discussed earlier,
"stress" is defined psychologically as any event which
challenges the organism's current level of
adaptation. Divorce, being laid off, or losing a
close friend are examples. Exposure to
unpredictable and uncontrollable aversive events is
inherently stressful. Even positive events can be
stressful, though they rarely play a role as instigators
of PTSD.
Documented exposure to trauma, as defined in DSM,
is necessary for the diagnosis of PTSD. But it is
not sufficient. Most people -- perhaps as many as
95% -- who are exposed to trauma do not develop PTSD
(Bonanno, 2011). This is true even when the
exposure is prolonged or severe.
However, some clinicians diagnose PTSD even in the
absence of such documentation, in patients who "have the
symptoms" of PTSD. Sometimes, the clinician
assumes that the patient has "repressed" or
"dissociated" his memory for the traumatic event.
It's as if they figure, "They have the symptoms, so they
must have been traumatized". But this is backwards
reasoning -- technically, the error of asserting the
consequent discussed in the lectures on Thought
and Language. In fact, patients can show
some of the symptoms of PTSD even in the absence of
exposure to trauma: for example, hyperarousal is
symptomatic of anxiety disorder, and poor sleep is
symptomatic of depression. Just because someone is
anxious and/or depressed doesn't mean that they've been
traumatized. They might be anxious or depressed for some
other reason. This error in reasoning was, in my view,
largely responsible for the "epidemic" of claims of
childhood sexual abuse that arose in the 1980s.
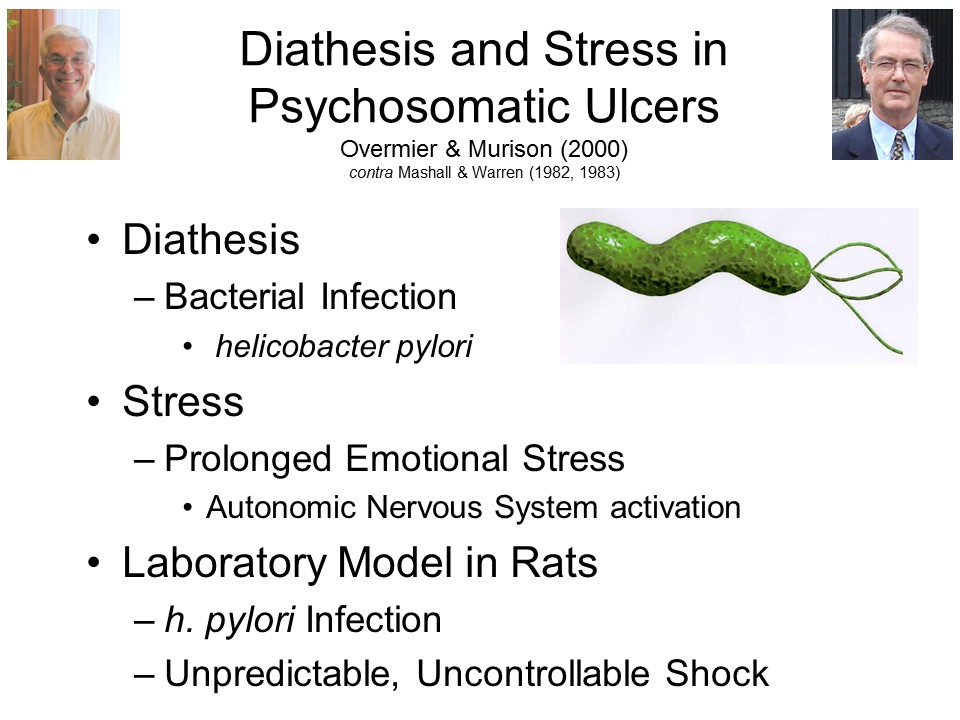
5. Psychosomatic Disorders
(also known as psychophysiological disorders)
involve actual damage to some organ enervated by the autonomic
nervous system, usually associated with psychological stress.
So-called psychosomatic ulcers are the classic
example: here, peptic ulcers of the stomach (gastric
ulcer) or small intestine (duodenal ulcer) occur in the
context of high levels of psychological stress.
"Type A" behavior -- very high levels of stress,
usually self-imposed through a regime of high activity
levels, aggressiveness, and competitiveness -- has been
associated with increased risk of coronary heart
disease.
Other instances of anatomical damage or physiological
malfunction may also be stress-related, as when stress
leads to a breakout of acne or a temporary disruption of
the menstrual cycle. Of course, both acne and dysmenorrhea
can have purely physical causes, but sometimes they do
occur under conditions of stress (like prom night).
6. Somatoform
Disorders are characterized by physical complaints that
have no organic basis. In this respect they are similar to the
dissociative disorders, except that the symptoms mimic
conditions arising outside the nervous system.
In hypochondriasis, the patient is excessively
concerned with the risk or threat of disease.
Somatization disorder (also sometimes known as Briquet's
syndrome or just plain "hysteria", involves
multiple, constantly changing physical complaints.
Somatoform pain disorder is characterized by
constant, frequent complaints of pain in various body
parts, in the absence of any evidence of a physical
condition that could cause this pain.
Body dysmorphic disorder is characterized by an
excessive concern that particular features of the body,
such as one's nose or ears, are "not right". Individuals
with body dysmorphic disorder are commonly found in the
waiting rooms of plastic surgeons, many of whom are only
to happy to have them as returning customers. Somehow,
though, the problem never seems to get fixed.
A controversial case is irritable bowel syndrome,
in which the patient experiences abdominal pain, cramping,
bloating, diarrhea, and constipation. Aside from these
symptoms, physical examination doesn't typically reveal
inflammation or other damage to the colon or other parts
of the gastrointestinal system -- leading some authorities
to suggest that it is a form of somatization disorder. On
the other hand, it could be a physical illness, perhaps
stress-induced, whose underlying pathology is still
unknown. Or, it could be a straightforward physical
illness, whose etiology has nothing to do with stress.
Something similar could be said about chronic
fatigue syndrome (CFS), where the patient suffers
from profound exhaustion, disordered sleep, and pain in
the muscles and joints -- sometimes so severe that the
patient cannot get out of bed, or engage in his or her
normal physical activities. Again, the frequent absence of
physical findings has led some authorities to suggest that
CFS is a somatoform disorder -- "all in the patient's
head", or perhaps depression masquerading as a physical
illness. But, as with IBD, this assertion is highly
controversial, and there are reputable medical researchers
who suspect that CFS stems from an underlying, if still
unknown, viral infection, or perhaps a form of autoimmune
disease.
7. Dissociative Disorders,
including conversion disorders, in which there is a
disruption of conscious awareness and control.
In the dissociative disorders, such as
dissociative amnesia (also known as functional
or psychogenic amnesia),
dissociative fugue (also known as psychogenic
fugue), and
dissociative identity disorder (also known as multiple
personality disorder), the dissociation affects
conscious awareness of identity and autobiographical
(episodic) memory.
In the conversion disorders, traditionally
collected under the rubric of hysteria, the
dissociation affects sensory-perceptual awareness
as in psychogenic or functional blindness,
deafness, or
anesthesia),
and/or the voluntary control of action (as in psychogenic
or functional paralysis).
The dissociative and conversion
disorders sometimes mimic the effects of damage to the
peripheral or central nervous systems, but in these syndromes
there is no evidence of brain insult, injury, or disease.
8. Personality
Disorders (e.g., borderline personality, antisocial
personality or psychopathy) are deeply ingrained --
longstanding, inflexible, and pervasive -- patterns of
maladaptive behavior which typically develop in adolescence.
In contrast to the psychoses and neuroses, whose symptoms are
"ego-dystonic" (experienced as alien and unwanted), the
symptoms of personality disorders are "ego-syntonic" --
experienced as a part of their normal personality.
In antisocial personality disorder (also known
as psychopathic personality disorder,psychopathy,
or sociopathy, the person engages in a pattern of
incorrigible antisocial behavior.
In borderline personality disorder (BPD), the
person experiences a blurring of the boundaries between
self and other, difficulty managing affect, etc. The
term "borderline" was coined by Adolph Stern to label
patients who seemed to fall in the cracks between neurosis
and psychosis. It was brought into the official
diagnostic nomenclature by John Gunderson, who identified
six characteristic features of the disorder (for more on
BPD, see "The Long Shadow of Trauma" by Diana Kwon, Scientific
American, 01/2022; but be wary of Kwon's hypothesis
that trauma lies at the origin of BPD as well as PTSD;
there's a kind of "trauma industry" among some mental
health professionals, which sees trauma everywhere and as
the cause of everything):
Intense emotions, especially anger and/or depression;
Impulsive behavior;
Brief episodes of psychosis;
Chaotic interpersonal relationships;
Illogical, loose, or bizarre thinking (itself a
characteristic of schizophrenia, with which BPD patients
were often formerly diagnosed);
Outward appearance of normality (which, of course, in
psychoanalytic thinking, only shows how abnormal the
person is!).
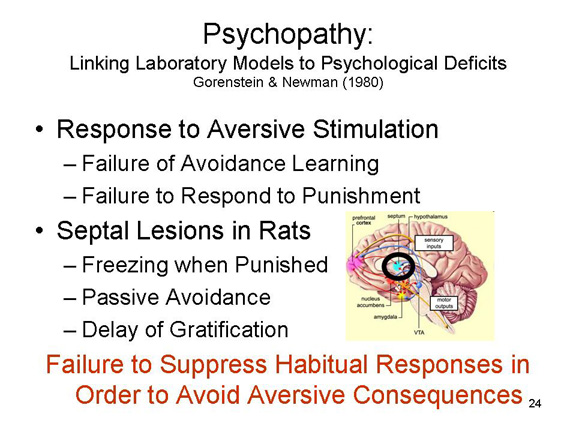
Psychopathy
The classical term for antisocial personality
disorder is psychopathy, first described by Philippe
Pinel, the French physician who famously freed the insane
from their chains, in 180, as mania without delirium,
because the patient did not display delusions or other
typical signs of psychosis. Later, Benjamin Rush, an
American physician who pioneered in the medical treatment of
the mentally ill, characterized the same syndrome as moral
derangement because violent and other antisocial
behavior featured so prominently in the cases he observed.
This term was replaced by moral insanity, and then
by psychopathy.
The classical clinical description of "primary
psychopathy" was provided by Hervey Cleckley's book The
Mask of Sanity (1941):
intelligent
charming
unreliable
dishonest
irresponsible
self-centered
emotionally shallow
lacking empathy
lacking insight.
These and symptoms were developed by Robert Hare, a Canadian
psychologist, into the Psychopathy Checklist (PCL), which has
become the standard instrument for assessing psychopathy.
Hare's book,Without Conscience: The Disturbing World of the
Psychopaths Among Us (1993), is essentially an update of
Cleckley's book, reviewing a considerable body of scientific
research on the syndrome.
(Cleckley was also co-author, with Corbett
Thigpen, of The Three Faces of Eve, a classic case
study of multiple personality disorder that was made into
an Oscar-winning film starring Joanne Woodward.)
There are also "secondary" or "neurotic"
psychopaths, whose antisocial behavior occurs in the context
of conflict and anxiety. One classic case of neurotic
psychopathy is Robert Lindner's Rebel Without a Cause:
Hypnoanalysis of a Criminal Psychopath, which -- I
swear this is true -- was made into the famous movie
starring James Dean, Natalie Wood, and Sal Mineo.
Cleckley's characterization of psychopathy is
summarized by John Seabrook in "Suffering Souls: The Search
for the Roots of Psychopathy" (New Yorker,
11/10/2008, p. 67):
"Beauty and ugliness, except in a very
superficial sense, goodness, evil, love, horror, and humor
have no actual meaning, no power to move him," Cleckley
wrote.... The psychopath talks "entertainingly,"... and is
"brilliant and charming," but nonetheless "carries
disaster lightly in each hand." Cleckley emphasized his
subjects' deceptive, predatory nature, writing that the
psychopath is capable of "concealing behind a perfect
mimicry of normal emotion, fine intelligence, and social
responsibility a grossly disabled and irresponsible
personality." This mimicry allows psychopaths to function,
and even thrive, in normal society.
In the 1930s, the alternative label psychopath
was coined by G.E. Partridge, and psychopathy entered the
first edition of the DSM as sociopathic
personality. In the 2nd edition of DSM, the
syndrome was renamed antisocial personality disorder.
Actually, psychopathy is quite not the same thing as
antisocial personality disorder. Only a minority of
individuals with the diagnosis of antisocial personality
disorder are psychopaths, as defined by Cleckley and Hare.
Psychopaths would seem to be excellent
candidates for the insanity defense -- after all, they
suffer from a particular mental disorder which, by its very
definition, disposes them to antisocial and criminal
behavior. Unfortunately, psychopathy is generally
excluded from the insanity defense from other
considerations. Not the least of which is that most
psychopaths, when asked will freely admit that their conduct
is immoral or illegal or unethical. So they do
appreciate the difference between right and wrong. And
in other respects, they can appear quite intelligent and
charming. They don't hallucinate, they're not
delusional. So, to all outward appearances, they would
seem both to understand the difference between right and
wrong and to be able to conform their conduct to societal
rules. But they don't and that makes them look like
they're criminals, not mentally ill. And they're
treated as such: it's been estimated that as many as 1/4-1/3
of prisoners in American jails are psychopaths.
9. Behavioral
Disorders consist of specific maladaptive behaviors that
occur in the absence of signs of any associated mental
disorders (e.g., psychosis, neurosis, or personality
disorder).
Alcoholism and alcohol abuse is a widely
recognized form.
Drug addiction and other forms of substance abuse
are also classified under this label.
Addictions to sex, gambling, and other activities
are also recognized as behavioral disorders. Whether these
are "real" addictions, like the physical addiction caused
by some drugs, is a matter of some controversy.
(10.) In
addition to these forms of mental illness, there are more
mundane problems in living (a phrase coined by T.S.
Szasz, a famous critic of psychiatry, in his book The Myth
of Mental Illness). These include:
marital stress
sexual dysfunction
adjustment problems
stress reactions
vocational quandaries.
These problems don't remotely resemble
mental illness, but they can be extremely distressing to the
people involved. Accordingly, they are often treated by mental
health professionals, including counseling psychologists as
well as clinical psychologists, psychiatrists, and clinical
social workers.
Culture-Specific Syndromes
Schizophrenia, depression
and anxiety disorder, like cancer, heart disease, and measles,
are found everywhere -- though their incidence and precise
manifestation can vary from culture to culture. While
this mean seem puzzling at first, the existence of
culture-specific syndromes only underscores the point that the
individual's mind and behavior exist in and are shaped by
sociocultural context, which is why psychology is both a
biological and a social science.
In addition, there are
certain forms of mental illness that are encountered only in
particular cultures. For example:
Latah, observed in Southeast Asia and Malaysia,
is characterized by sudden, extreme startle reactions,
loss of behavioral control, and profanity.
Ataque de nervios, observed in Latin America, is
characterized by shouting, tremors, cursing, feelings of
loss of control, and extremely high levels of fear, and
can be accompanied by interpersonal violence or suicidal
behavior.
In koro, observed in Southeast Asia and Africa,
the person is obsessed by the idea that his genitalia are
shrinking and disappearing.
In amok, observe din Malaysia, men (mostly)
withdraw and brood, followed by a bout of uncontrolled
violence -- hence the English phrase, "running amok".
In 2-D love, some Japanese men (again, mostly)
develop romantic infatuations with animated characters (anime).
These syndromes are rarely seen in
western developed countries -- except, perhaps, among recent
immigrants from these regions.
An interesting recent case is uppgivenhetsyndrom
("resignation syndrome"), which has been diagnosed among
refugee children in Sweden who face deportation -- only in
Sweden (at least so far), and only in refugee children (not
adults). These children (and, for that matter, their
parents) are under constant, prolonged stress -- first from
the conflict that made them refugees in the first place, then
from the difficult migration from their home country through
Europe to Sweden, and then from the uncertainties of refugee
life: How long will they be able to stay? How will
they live while they are here? When will they be able to
return home? What will things be like when they get
there? In fact, some refugees are denied asylum, even in
a country like Sweden, and it's in these children that uppgivenhetsyndrom
is diagnosed. A typical patient appears to be
unconscious, even comatose: “totally passive, immobile, lacks
tonus, withdrawn, mute, unable to eat and drink, incontinent
and not reacting to physical stimuli or pain.” However,
they are not in a coma. Their reflexes are normal, as
are cardiovascular signs such as pulse rate and blood
pressure. In fact, they show no signs of neurological or
any other physical illness. For this reason, even though
these children are obviously under a great deal of stress, uppgivenhetsyndrom
is not a stress-related psychophysiological disorder,
precisely because there is no evidence of any organic damage
-- as you would find in extreme cases of Selye's General
Adaptation Syndrome (discussed in the lectures on "The Biological Bases of
Mind and Behavior"). In our terms, uppgivenhetsyndrom
appears to be a culture-specific form of somatization
disorder. Cases started appearing in the early 2000s,
and by 2005 more than 400 cases had been diagnosed. The
children typically recover if their families are permitted to
stay in Sweden, especially if they (and their families) also
receive psychotherapy aimed at their underlying state of fear
and hopelessness (Bodegard, Acta Paediatrica, 2005;
see also "The Apathetic" by Rachel Aviv, New Yorker,
04/03/2017, which also discusses culture-specific syndromes in
general).
Cultural differences can also work in
reverse, preventing "universal" illnesses from being
recognized. The Hmong people of Laos recognize a
condition known as quag dab peg -- literally,
“the spirit catches you and you fall down”; it is treated
through religious rituals. In the West, this same
condition is known as epilepsy, and is usually treated quite
effectively with drugs. For an excellent treatment of
this problem among Hmong refugees in the Unites States, see The
Spirit Catches You and Then You Fall Down: A Hmong
Child, Her American Doctors, and the Collision of Two
Cultures by Anne Fadiman (1997).
Although there are some culture-specific
forms of mental illness, for the most part the major
psychiatric syndromes are considered universal. In Crazy
Like Us: The Globalization of the American Psyche
(2010), Ethan Watters argues that DSM has become a
kind of cultural export, shaping non-Western views of mental
illness and its treatment. Watters suggests that this is
a bad thing -- a kind of intellectual colonialism. On
the other hand, nobody complains when other aspects of Western
science and medicine are exported to non-Western countries, as
in the case of treatments for HIV/AIDS, Ebola, or Zika.
It's likely that schizophrenia, depression, anxiety, and other
major mental illnesses are, indeed universal. But still,
non-Western countries likely have something to teach us about
prevention and treatment. For example, epidemiological
studies have found that the prospects for recovery from
schizophrenia are much better in some cultures than others -
-suggesting that, when it comes to mental illness, it's not
all in the genes and neurotransmitters.
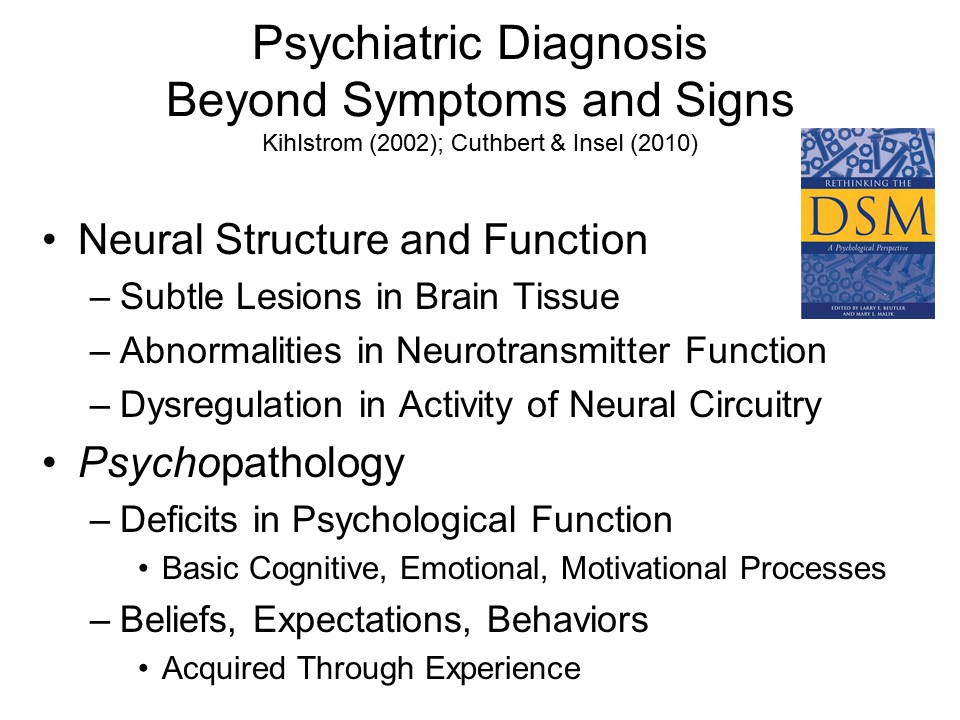
Structure and Function
In many ways, mental
illnesses are analogous to the physical illnesses diagnosed
and treated by physicians and other medical professionals.
Just as physical illness stems from abnormalities in bodily
structure or function -- a weak heart valve, or bacterial
infection, or whatever -- so mental illness stems from
abnormalities in mental structure or function -- a
defect in the system for affect regulation, perhaps, or just
acquiring, through learning, some maladaptive belief or
expectation.
Abnormalities in cognition are prominent in Alzheimer's
disease and other forms of dementia, and in schizophrenia.
Abnormalities in emotion are prominent in the anxiety
disorders, and in the affective disorders.
Abnormalities in motivation are prominent in
psychopathy.
The Medical Model of Psychopathology
In fact, the language of medicine pervades
our discussion of psychopathology. Thus, we have:
mental patients,
with acute mental illnesses,
associated with a particular etiology,course,
and prognosis,
treated in mental hospitals,
which also have rehabilitation programs for the
chronically mentally ill, and
programs of mental hygiene to prevent mental
illness from occurring in the first place.
Mental illness is diagnosed
by
symptoms, or publicly observable manifestations
of psychopathology (as when a patient complains about
being depressed), and
signs, manifestations of psychopathology that are
identifiable by a trained professional (perhaps by the
results of formal psychological testing).
These symptoms and signs
of mental illness may be grouped into
syndromes, or clusters of symptoms that tend to
occur together;
diseases, which are syndromes whose underlying
cause is known; and
illness, which is the subjective experience of
disease
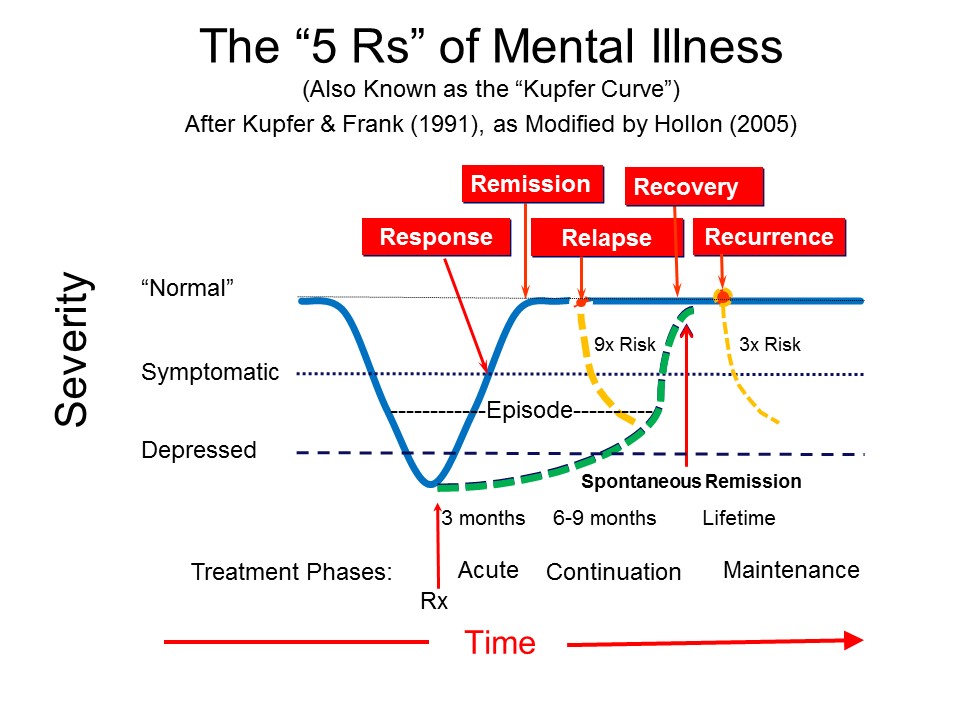
Mental illnesses run a particular time course:
There is an acute phase, between the onset of
illness and its remission (whether the illnesses
is treated or not).
If the illness does not remit, the patient proceeds to
the chronic phase.
Prognosis refers to the likelihood that remission
will improve (with treatment or not).
Relapse refers to a return of symptoms after a
patient has shown some improvement.
Recurrence refers to a new acute episode of
illness after a patient has achieved remission.
These analogies are one aspect of the medical
model of psychopathology.
Beyond these
analogies, the medical model also has implications for the
nature of mental illness. However, these implications are
commonly misunderstood. It is commonly believed that the
medical model ascribes mental illnesses to organic causes.
That every psychiatric syndrome is ultimately an organic brain
syndrome. As Ralph Gerard, one proponent of this viewpoint,
once put it:
"Behind every twisted thought there lies
a twisted molecule".
Similarly, Eric Kandel, the psychiatrist
who won the Nobel Prize for his studies of long-term
potentiation in Aplysia, discussed in the lectures on "Learning", has stated
that "All mental processes are brain processes, and therefore
all disorders of mental functioning are biological
diseases.... The brain is the organ of the mind.
Where else could [mental illness] be if not in the brain?"
(quoted by Kirsten Weir in "the Roots of Mental Illness", Monitor
on Psychology, 06/2012).
This "somatogenic" view of mental
illness is quite popular, but it is not what the medical model
is about. All the medical model asserts is that mental illness
has natural causes.According to the medical model, the
causes of mental illness may be biological in nature, or they
might be psychosocial in nature. All that matters is that they
are natural causes that can be ascertained through the methods
of empirical science -- namely psychology and related fields.
By extension, the medical model holds that mental illness can
be treated and prevented by methods derived from scientific
research.
Misunderstanding the Medical Model
However, there are considerable
misunderstandings abroad about the nature of the medical model
-- including misunderstandings perpetrated by many writers of
introductory textbooks in psychology. For example, the 4th
edition Gleitman's Psychology (1995, p. 722), the book
that I have used most often in teaching introductory
psychology, described the medical model as follows:
Some authors endorse the medical model, a
particular version of the pathology model [which assumes
that symptoms are produced by an underlying pathology, and
that the main goal of treatment is to discover and remove
this pathology], that assumes... that the underlying
pathology is organic. Its practitioners therefore employ
various forms of somatic therapy such as drugs. In
addition, it takes for granted that would-be healers
should be members of the medical profession.
Many other introductory textbooks (as
well as texts in abnormal and clinical psychology) have
similar passages. For the most part, they are intended to
distinguish an ostensibly somatogenic medical model from the
psychogenic models associated with cognitive and behavioral
therapy, or to distinguish the profession of psychiatry, with
its emphasis on drugs and other physical treatments, from
clinical psychology, with its emphasis on behavioral
interventions. This common association of the medical model
with somatogenic theories and biological treatments reflects a
deep misunderstanding, and what I have presented here follows
is an attempt to give an alternative perspective on this
issue, based on Siegler and Osmond's (1974b) sociological
analysis of the medical model,Models of Madness, Models of
Medicine (see also Shagass, 1975).
Interestingly, the Osmond of Siegler &
Osmond is Humphrey Osmond (1917-2004), a pioneering LSD
researcher who (in 1957) coined the word psychedelic
to describe the effects of that and other hallucinogenic
drugs. Osmond gave LSD to Aldous Huxley, who wrote The
Doors of Perception about the experience -- a book
from which the rock group The Doors, led by Jim
Morrison, took their name. Initially, Osmond thought that
LSD would serve as a laboratory model (see below) of
schizophrenia (or, at lest, of schizophrenic
hallucinations), but he later focused his attention on the
potential of it and other psychedelic drugs to treat
alcoholism and promote "transcendent" alterations in
consciousness (Osmond's obituary appeared in the New
York Times, 02/22/04).
According to Siegler and Osmond, the
history of psychology can be traced in terms of three major
models of psychopathology. The supernatural model
prevailed before the 18th century Enlightenment. It assumes
that psychology reflects the possession of the individual by
demons; by implication, the proper response to psychopathology
is exorcism. The moral model, which prevailed in the
late 18th and early 19th centuries, assumes that
psychopathology -- or, more precisely, abnormal behavior -- is
deliberately adopted by the individual, much in the manner of
criminal behavior; by implication, the proper response to
psychopathology is confinement and other forms of punishment.
The medical model, which began to emerge in the 19th
century, assumes only that psychopathology is the product of
natural causes that can be identified by the techniques of
empirical science. By implication, the proper response to
psychopathology is diagnosis according to a scientifically
validated system, and attempts at cure or rehabilitation by
means of scientifically proven methods. Contrary to the
popular view, the medical model does not assert that
psychopathology is the product of an abnormal biological
condition, or that it should be treated only with drugs or
surgery. Rather, the medical model is centered on particular
rules regulating two primary social roles: the doctor and the
patient.
To illustrate the differences between
these models, consider the 1973 decision by the American
Psychiatric Association, to "de-list" homosexuality as a
mental illness. As Charles Silverstein (2011) has noted -- he
was one of the psychologists who persuaded the psychiatrists
to change their position -- at the time, "homosexuality was
considered a crime, a sin, and a mental pathology". So, in
that case, homosexuality fell under both the supernatural
model (it was considered to be a sin, the work of the Devil),
the moral model (it was considered to be a crime, a willful
antisocial act), and it was considered to be an illness (a
sexual pathology).
The doctor (who does not have
to be a physician, or even hold a doctoral degree) possesses a
special kind of authority called Aesculapian (after
Aesculapius, the Greek god of medicine). Aesculapian authority
is a combination of three other kinds of authority recognized
by sociologists:sapiential authority, by virtue of the
doctor's special knowledge and expertise;moral
authority, by virtue of the doctor's concern for the afflicted
individual; and charismatic authority, by virtue of
the afflicted person's faith that the doctor will be of help.
Note that doctors lack structural authority: they
cannot enforce their prescriptions, resulting in a markedly
low rate of compliance. The doctor's role is to investigate
the disorder at hand, by means of procedures that might be
unpleasant, intrusive, or even frightening. On the basis of
this investigation the doctor makes a diagnosis, informs the
afflicted person about the nature of his or her problem,
absolves the patient of blame (it is critical to medical
ethics that people are not blamed, and thus punished, for
their illnesses), and finally creates the conditions for the
afflicted person to return to health and his or her proper
role in society.
The patient enacts his or her
part by taking on the sick role: he or she must seek
help from the doctor, and cooperate with treatment; in return,
the patient is exempt from some or all of his or her
responsibilities during treatment. Note that a doctor's order
has supreme authority in society -- it can exempt the person
from jury duty, military service, and final examinations. It
has this power by virtue of our society's implicit adoption of
the medical model and the sick role. However, patients cannot
remain in the sick role forever: they must leave it
eventually, either by recovering or dying.
A special case is when the illness is
chronic, and nothing more can be done to achieve a cure. Under
these circumstances the role relationships change. It is the
responsibility of the doctor to remove the sick role, and
confer the impaired role on the afflicted patient. At
this point the patient must leave the hospital and active
treatment. What once was an illness is transformed into a handicap;
and the doctor is replaced by a rehabilitation specialist.
Patients are no longer absolved from their responsibilities:
they must return to some socially productive activity, do
things for themselves, and cope with their handicaps as well
as possible.
What has just been
described is what Siegler and Osmond (1974) call the clinical
medical model, which is one of many different versions.
All versions of the medical model assume that disease is the
product of natural causes, and that the proper response is
scientifically based treatment. However, they differ in terms
of their role relationships. In the clinical medical model,
the goal is to cure disease in an individual, and the role
relationships are doctor and patient.
In the public health medical model, the goal is
to cure illnesses that cannot be controlled on an
individual basis. Its focus is on prevention of disease in
a population, rather than an individual, and in fact its
prescriptions for public health may damage some
individuals; moreover, the public health official may
decide to permit some diseases to occur, perhaps for
economic reasons. Note that the role relationships differ
in the public health medical model. The doctor is replaced
by the public health official, who has structural
as well as sapiential authority -- he or she has the power
of the law and the courts to enforce "doctor's orders",
and to force us to fluoridate our water, or be immunized
against smallpox and polio. And the patient is replaced by
the citizen, who by his or her vote can place
limits on the public health official's authority to act.
In the scientific medical model, there is no
direct interest in intervention (prevention or cure), but
interest only in the acquisition of scientific knowledge
about the nature of disease. Again, the role relationships
change. The doctor is replaced by the investigator
who has only sapiential authority. The investigator has no
obligation to cure and prevent disease, and in certain
circumstances may even inflict disease (or allow it to
occur) as part of a controlled experiment. The patient is
replaced by the subject who volunteers his or her
services. Subjects are under no obligation to participate
in research, and do so only when they are compensated in
some way for their services. Subjects have rights that
patients and citizens do not: they must be protected from
harm, and must be assured that the procedures to which
they are subjected are worthwhile; their only
responsibility is to honor their commitment to the study.
So much detail has been devoted to the
medical model because it has been subject to so much
misunderstanding -- and also because it gives us the
opportunity to unite two social sciences, psychology and
sociology, at least for a moment. However, the interested
reader should reflect on the implications of the medical
model(s) for understanding psychopathology -- its nature,
causes, treatment, and prevention. And also reflect on the
proposition that many of the abuses frequently attributed to
mental health professionals -- such as the confinement of
mental patients in the back wards of mental hospitals, without
any active treatment -- actually represent violations, not
expressions, of the medical model.
Excerpted from Kihlstrom, J.F. (2002), "To
honor Kraepelin...: From symptoms to pathology in the
diagnosis of mental illness". In L.E. Beutler & M.L.
Malik (Eds.),Alternatives to the DSM (pp. 279-303).
Washington, D.C.: American Psychological Association.
Diagnosis as Categorization
The diagnosis of mental
illness is an act of categorization in which patients (or
their illnesses) are assigned to categories based on the same
feature-matching process we use to categorize other objects.
The patient's symptoms and signs serve as features.
The clinician compares the patient's symptoms and signs
to those that are associated with various diagnostic
categories, as listed in the Diagnostic and
Statistical for Mental Disorders (DSM),
published by the American Psychiatric Association. The DSM
is the "official" list of mental illnesses recognized by
the psychiatric profession in America, and has been
adopted by other helping professions, such as clinical
psychology and clinical social work, as well.
The patient's illness is diagnosed in terms of the
illness that most closely fits his or her symptoms.
Sometimes a patient receives more than one diagnosis, a
situation known as comorbidity. For example,
anxiety disorder is often "comorbid" with depressive
disorder.
There is a natural linguistic tendency to confuse the
patient with the illness -- that is, to refer to
"schizophrenics" and "depressives" instead of "patients
with schizophrenia" or depression. This transformation of
a category of illness into a category of people is
politically incorrect, and a source of great annoyance to
many mental patients and their families. But we can't
really help engaging in such linguistic shorthand, anymore
than we can help referring to people as "Asians" or
"Hispanics" -- or, for that matter, "extraverts" or
"homosexuals".
Formal psychiatric diagnosis essentially
began with a French physician, Jean-Etienne Dominique Esquirol
(1772-1840), who drew a fundamental distinction between the
insane, the mentally deficient (today we use the term intellectually
disabled), and the criminal. In the 19th century, Emil
Kraepelin (1856-1926) divided the psychoses into two major
categories --dementia praecox (early dementia, or what
we now call schizophrenia) and manic-depressive illness
(what we now call affective disorder). And a little later,
Pierre Janet (1859-1947) did for the neuroses what Kraepelin
had done for the psychoses, dividing them into two major
categories --hysteria (including what we now call the
dissociative and conversion disorders) and psychasthenia
(including anxiety disorders and some forms of depression).
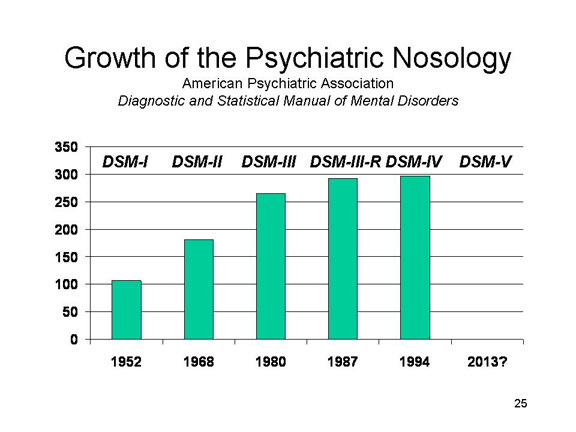
Since
the 19th century, the number of recognized mental illnesses
has grown markedly. The first edition of the Diagnostic
and Statistical Manual for Mental Disorders (DSM-I),
published in 1952, listed only about 100 different syndromes.
The latest edition,DSM-V, published in 1994, listed
almost 300.DSM-VI is due to be published sometime
around 2012, and we'll see how many mental illnesses there are
then!
Whatever its edition,DSM is
essentially a catalog of mental illnesses, with a list of the
symptoms characteristic of each. Diagnosis is essentially a
feature-matching process that asks whether a patient has the
symptoms associated with a particular syndrome or disease. In
other words, diagnosis is an act of categorization, so it is
interesting to look at what kind of categories the diagnostic
categories are.
Diagnostic Categories as Proper Sets
In the past, the
diagnostic categories of mental illness were at least tacitly
construed as proper sets, where sets of symptoms served as
defining features of a syndrome, singly necessary and jointly
sufficient to define an illness (such as schizophrenia) or a
person (such as a schizophrenic) as having some illness.
For example, traditionally mental illnesses were
classified as organic (associated with
demonstrable brain insult, injury, or disease) or functional
(occurring in the absence of obvious brain damage).
The functional mental illnesses were also
characterized as psychotic (featuring a loss of
reality testing) or neurotic (featuring symptoms
of anxiety).
The functional psychoses were classified (by Ernst
Kraepelin, a 19th-century psychiatrist) into two broad
groups,dementia praecox (what we now call
schizophrenia, featuring symptoms of cognitive
disorder) or manic-depressive illness
(featuring symptoms of affective disorder).
The neuroses were also classified (by Pierre Janet,
another psychiatrist of the late 19th and early 20th
century) into two broad groups,psychasthenia
(syndromes such as anxiety disorder, obsessive-compulsive
disorder, hypochondriasis, and "neurotic" depression,
where the patient is aware of what is wrong), and hysteria
(such as psychogenic amnesia, blindness, or paralysis)
where the patient suffers a constriction in awareness.
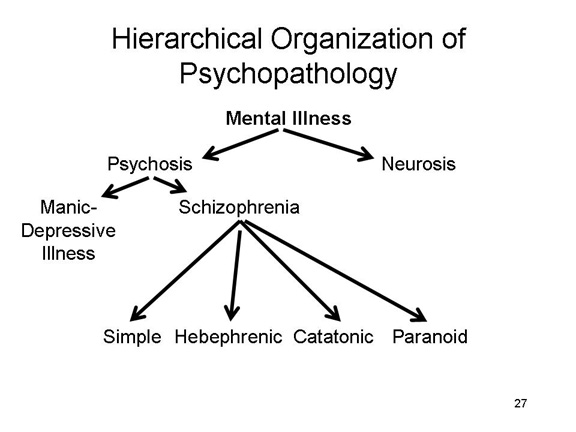
In this way, the
traditional psychiatric nosology formed a conceptual hierarchy
with superordinate categories (organic vs. functional,
psychotic vs. neurotic) at the top. Subordinate categories
were then created by adding symptoms (such as loss of reality
testing or problems with anxiety) as defining features.
The Case of Schizophrenia
The nature of traditional
psychiatric diagnosis, as a perfectly nested hierarchy of
proper sets, is exemplified by the work of Eugen Bleuler, a
Swiss psychiatrist who in 1911 redefined dementia praecox as
"the group of schizophrenias".
Bleuler accepted Kraepelin's classification of "dementia
praecox" as a functional psychosis; but he did not
believe, as Kraepelin's name implied, that the syndrome
was merely a form of dementia that occurred relatively
early in life, as opposed to the "senile dementia"
associated with old age.
Instead, Bleuler believed he had discovered a new form
of illness characterized by a discordance among basic
mental faculties of cognition, emotion, and motivation --
hence his label,schizophrenia.
In Bleuler's view, all schizophrenics shared four
symptoms in common -- his "Four As":
associative disturbance, manifested in a
certain disorganization in the logical organization of
thought ("thinking crookedly"), neologisms (made-up
words), "word salad" consisting of loose, "clang", and
chained associations, and a tendency toward
over-inclusiveness in categorization;
anhedonia, an inability to experience positive
emotions -- and, more generally,blunted or inappropriate
affect (emotional responses that are not correctly
tuned to the situation);
ambivalence, a lack of initiative and a
diminished motivation to comply with others' wishes; and
autism, withdrawal from others and a general
detachment from reality.
There were also four subtypes, characterized by
additional defining symptoms:
simple, as described above;
hebephrenic, characterized by childlike
demeanor;
catatonic, characterized by immobility; and
paranoid, characterized by delusions.
Bleuler clearly construed
the 4 As as defining features of schizophrenia:
Every schizophrenic patient displayed all four symptoms
in one form or another.
Every patient who displayed all four symptoms was a
schizophrenic.
The boundaries between schizophrenia
and manic-depressive illnesses were clear: you could have one
illness or the other, but not both. And the boundaries between
schizophrenic subtypes were also clear: you could be
hebephrenic or catatonic, but not both.
A similar hierarchy of syndromes
developed around manic-depressive illness.
Problems with the Diagnostic Categories
This view of the diagnostic categories
as proper sets, recognized by symptoms that were singly
necessary and jointly sufficient to define the diagnosis. And
early editions of the DSM were at least implicitly
structured around this conceptualization, in terms of the
"textbook cases" it used to characterize each syndrome.
However, the traditional
view quickly encountered problems of a sort that are familiar
from the critique of the classical view of categories as
proper sets (discussed in the lectures on Thought and
Language).The simple fact was that very few patients actually
resembled the textbook descriptions of the various syndromes.
Partial Expression: Many patients displayed some
but not all of the symptoms that defined a particular
syndrome. In the case of schizophrenia, this led to the
introduction of new syndromes such as schizoid
personality disorder,schizotypal personality
disorder, and paranoid personality disorder.
There were also many different forms of depression.
Combined Expression: Many patients displayed
defining symptoms of several different categories. In the
case of schizophrenia, again, this led to the introduction
of new syndromes such as pseudoneurotic schizophrenia,pseudopsychopathic
schizophrenia,schizoaffective disorder. The
term borderline personality disorder was
introduced to cover patients who displayed the symptoms of
both psychosis and neurosis -- they were literally "on the
border" between these major diagnostic categories.
Psychiatric Syndromes as Fuzzy Sets
Accordingly, for the third
edition of DSM (DSM-III), published in 1980,
the diagnostic system was reformed to take into account a new
understanding of the structure of natural categories offered
by cognitive psychology. Under this "revisionist" view:
The diagnostic categories were construed as fuzzy sets,
rather than proper sets: there is no clear boundary that
distinguishes schizophrenia or anxiety disorder from other
forms of mental illness.
Symptoms are considered to be characteristic rather than
defining features, only probabilistically associated with
various syndromes: delusions may be highly likely to occur
in schizophrenia, but they do not define schizophrenia
because they are also observed in other syndromes.
Specific instances of the categories sharing a family
resemblance, resulting in a great deal of heterogeneity
among patients carrying the same diagnosis.
Each syndrome is represented by a "prototypical" patient
who has many, but not necessarily all, of its
characteristic symptoms.
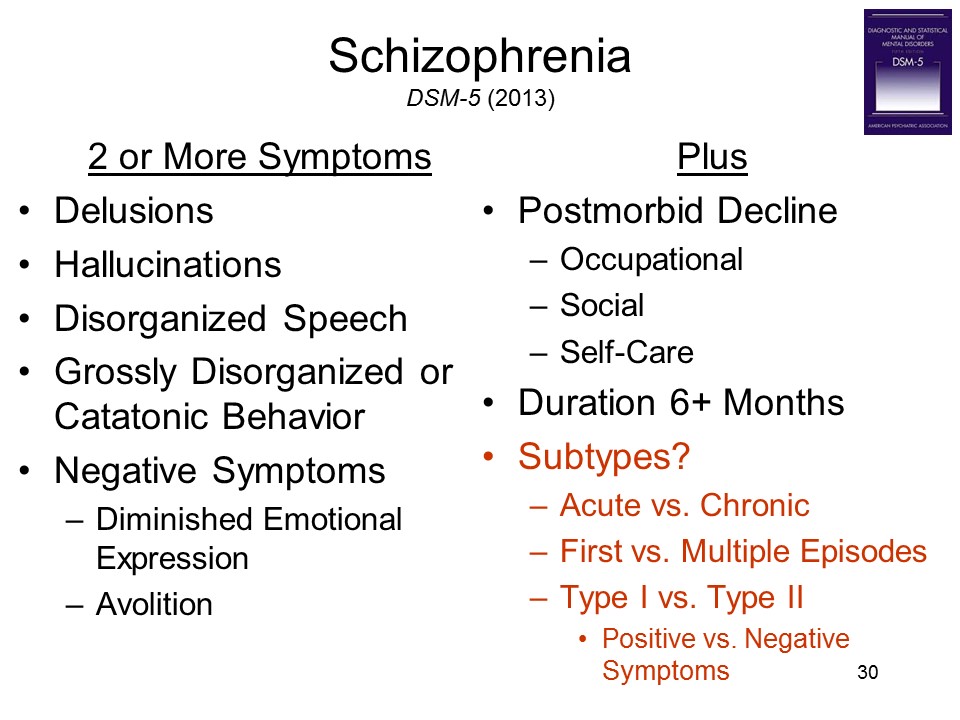
Consider, for example, several
prominent psychiatric diagnoses, as listed in DSM-5
(2013):
Schizophrenia may be
diagnosed in the presence of any two
"characteristic symptoms". Positive symptoms
entail the presence of something normally absent,
like delusions.Negative symptoms entail the
absence of something normally present, appropriate
emotional responses.
One patient may have delusions and
hallucinations while another may have catatonic
behavior and flat affect, but both are
"schizophrenics".
DSM-5 also abandons the
Bleulerian subtypes, such as hebephrenic and
catatonic schizophrenia, in favor of a distinction
between acute and chronic schizophrenia, and whether
the patient has had multiple episodes prior to the
current one. Some clinicians and researchers
promote a distinction between Type I
schizophrenia, where positive symptoms predominate,
and Type II schizophrenia, dominated by
negative symptoms.
Similarly, Major Depressive
Disorder can be diagnosed after observing any
five of a large number of symptoms. Note that
depression can be diagnosed even if the person
doesn't feel depressed (!), so long as he does
manifest diminished interest or pleasure in most or
all daily activities.
All patients with Anxiety
Disorder must display abnormal levels of
anxiety, but this singly necessary symptom is not
sufficient to make the diagnosis. Other symptoms
must also be present, but none of these additional
symptoms is necessary for the diagnosis.
Similarly, the diagnosis of Post-Traumatic
Stress Disorder requires that the patient have
been exposed to traumatic levels of stress, so this
is another instance of a singly necessary defining
feature. The exposure may take the form of directly
experiencing, or "just" witnessing, the trauma; or
learning about a trauma which occurred to a
significant other. The exposure can also be
repeated or prolonged, not just a single
episode. But none of the other symptoms are
necessary to make the diagnosis. The patient must
show some "intrusion" symptoms, as well as
symptoms of avoidance, negative alterations of
cognitions or mood associated with the trauma, and
marked alterations in arousal and reactivity, so
these criteria also have some of the qualities of
necessary symptoms. But there are lots of
different ways to display these features, no
particular manifestation is necessary.
A statistical technique called network
analysis can be used to show the relations among the
various categories of psychopathology. Denny Borsboom, a Dutch
psychologist, and his colleagues created a simple spreadsheet
showing the co-occurrence of all the symptoms listed in DSM-IV
-- that is, how many times insomnia and fatigue are listed as
characteristic symptoms of the same syndrome (such as sleep
disorder or depression). The obtained a graph in which each
symptom is represented by a node, and nodes are connected
whenever two symptoms are characteristic of the same disorder.
They then colored each of the nodes, according to the major
category of mental illness in which each symptom occurred. The
resulting graph shows the extent of symptom overlap in DSM-IV.
in which
Regardless of diagnostic category, there
was no expectation that all of the symptoms listed under a
syndrome will be present in any particular case. In principle,
we can observe all possible combinations of characteristic
symptoms. Diagnosis, then, is a matter of judgment under
uncertainty. Studies of the diagnostic process by Nancy
Cantor and her associates show that the certainty with which a
diagnosis of schizophrenia is made, for example, will be a
function of the number of the patient's symptoms that are
highly characteristic of schizophrenia, and the number of
symptoms that are more characteristic of other diagnostic
categories. In this system, "textbook cases" serve as category
prototypes, and there is explicit recognition of heterogeneity
among actual patients.
DSM-5
The Diagnostic and Statistical
Manual for Mental Disorders (DSM) was
first published in 1952, with a second edition appearing in
1968. Both manuals were as much literary productions as
scientific ones. They were heavily influenced by
Freudian psychoanalysis, centered on the distinction between
psychoses and neuroses, and didn't really include clear
criteria for making various diagnoses. All that changed
with DSM-III in 1980 (a revised edition, known
as DSM-II-TR, for "Text Revision", came out in 1987),
and DSM-IV in 1994. In these editions, serious effort
went into producing checklists of symptoms by which the
various disorders could be reliably diagnosed.
The fifth edition of DSM,
known as DSM-5, retains the "fuzzy set" structure of
the diagnostic categories, while sometimes revising the
criteria for specific disorders.
For example, in DSM-IV, the diagnosis of
schizophrenia required the presence of any two
"characteristic symptoms", whether positive or
negative. In DSM-5, the diagnosis requires
that at least one of these "characteristic symptoms" be a
"positive" symptom such as delusions, hallucinations,
disorganized speech, or grossly disorganized behavior.
Moreover, it abandons the Bleulerian" subtypes of
simple, hebephrenic, catatonic, and paranoid
schizophrenia.
DSM-IV diagnosed autism based on three criterial
symptoms: impairments in social interaction, impairments
in social communication (language), and restricted,
repetitive, and stereotyped patterns of behavior,
interests, and activities. DSM-5 lumps the
two kinds of social impairments together, so that
Asperger's syndrome joins classic autism in a single
category ofautistic spectrum disorder.
The implication is that autism and Asperger's syndrome
differ only in degree, quantitatively, not in kind,
qualitatively. Many in the autism/Asperger's
community disagree, including Temple Grandin, whose
vigorous critique-from-the-inside of DSM-5 is
included in her 2013 book, the Autistic Brain:
Thinking Across the Spectrum (2013, written with
Richard Panek).
However, DSM-5 abandons
certain other features of previous editions.
Previous editions were arranged hierarchically, with
major sections devoted to the psychoses, mood disorders,
anxiety disorders, and the like. DSM-5 is
organized developmentally, with the earliest chapters
covering disorders that first appear in
childhood.
Reflecting increasing cultural diversity, DSM-5
pays more attention to "culture-specific" syndromes, as
well as cultural factors that may affect diagnosis.
Earlier editions made liberal use of a subcategory Not
Otherwise Specified (NOS), as in "Psychotic
Disorder -- Not Otherwise Specified", for use with
patients who displayed some features of psychosis, but not
enough to enable a more specific diagnosis. Previously, a
remarkably high proportion of psychiatric patients
received diagnoses containing the NOS suffix. This
was especially true of the personality disorders and
pervasive developmental disorder (autism). NOS allowed
psychiatrists too much leeway to diagnose anyone
with a mental illness, without being specific as to
precisely what illness he or she had: the suffix is now
gone.
At the same time, DSM-5 also allows
practitioners to assess a disorder's degree of severity in
the particular patient -- much as medical disorders are
rated as mild, moderate, or severe. So, a patient could
meet all the criteria for schizophrenia, even though each
of the relevant symptoms was present only to a mild or
moderate degree.
Previous editions classified patients according to
several "axes".
Axis I referred to the mental disorder itself, such as
schizophrenia or bipolar disorder.
Axis II referred to background personality
characteristics, and included the personality disorders
themselves, as well as intellectual disability.
Axis III concerned general medical conditions that
might relate to diagnosis or treatment.
Axis IV referred to socioeconomic factors, such as
poverty, that might be relevant to diagnosis or
treatment.
Axis VI consisted of a global assessment of
functioning.
Aside from Axes I and II, none of these dimensions
got much use in real-world, everyday diagnosis, and so they
were dropped.
Some of the changes in DSM-5
are highly controversial.
Although it eliminates the NOS subcategory for specific
mental disorders such as schizophrenia, it includes a new
category of Unspecified Mental Disorder,
specifically for patients who "do not meet the full
criteria for any mental disorder" (p. 708).
And it also revives NOS in another guise, as in the
new category of Unspecified Schizophrenia Spectrum
Disorder and Unspecified Attention
-Deficit/Hyperactivity Disorder.
DSM-5 collapses Autistic Disorder and Asperger's
Syndrome into a single category of Autistic
Spectrum Disorder. The implication is that
Asperger's Syndrome differs from Autistic Disorder only in
terms of severity. But autism and Asperger's Syndrome
don't just differ quantitatively, in terms of severity.
They also differ qualitatively, in that patients with
Asperger's Syndrome have language abilities that patients
with Autistic Disorder simply don't have. Moreover, people
with Asperger's Syndrome have an interest in interpersonal
relations, even if they lack the skills to build or
maintain them. Classifying a child with Asperger's
Syndrome as "autistic" may mean that the child will not
receive optimal treatment.
As another example, DSM-5 eliminates the "bereavement
exclusion" for the diagnosis of Major Depressive
Episode. Previously, people who showed signs of depression
immediately following the loss of a loved one (spouse,
child, parent, pet, friend, etc.) were not diagnosed as
"depressed" unless their depression continued for more
than two months after the onset of symptoms. But
now, patients can be diagnosed as "depressed" even though
they are still mourning a loss.
The diagnosis of bipolar disorder has come to be
used more frequently with children, a trend that is highly
controversial in itself. Compounding the
controversy, DSM-5 introduces a new diagnostic
category of disruptive mood dysregulation disorder
-- which, critics suggest, might apply to any child who
has frequent temper tantrums.
Bipolar disorder used to be a form of what Kraepelin
calledmanic-depressive illness, a broad
category which also included syndromes of "pure" mania
and depression. In classic MDI, patients
experienced alternating periods of mania and depression,
usually separated by a symptom-free interval. By
the time that DSM-III was published, however,
bipolar disorder was considered to be distinct from
depression; and there were so few cases of mania that it
was virtually written out of the diagnostic
manual. But DSM-5 now acknowledges a
number of subtypes: Bipolar I disorder (BP I)
includes patients with episodes of severe mania,
regardless of whether they have episodes of depression;
patients with Bipolar II (BP II) experience
milder episodes of mania (what is known as hypomania),
along with episodes of depression. Then there is a
separate category for unipolar depressive disorder;
but, so far, there is still no recognition of unipolar manic
disorder. For more on the status of mania
and manic-depressive disorder, see "The Undiscovered
Illness" by Simon Makin (Scientific American,
03/2019).
In addition to anorexia and bulimia, DSM-5
introduces the opposite side of the eating-disorder coin,
binge-eating disorder, applied to anyone who eats
to excess at least once per week.
Hoarding is now a full-fledged mental disorder in
its own right, not just one possible symptom of
obsessive-compulsive disorder.
Some commentators have expressed the
fear of diagnostic inflation -- that these kind of
changes may make it possible to diagnose anyone with a
mental illness -- or, at least, that DSM threatens to
"pathologize normality" by classifying normal mental states,
like bereavement or even shyness (which can resemble
depression), as mental illnesses. (Benjamin Wolman, a
leading psychoanalytic psychotherapist, once wrote a book
entitled Call No Man Normal.) Over-diagnosis, of
course, inevitably leads to over-treatment.
In addition, some of those responsible
for formulating the DSM-5 criteria had unacknowledged
links with the pharmaceutical industry, raising the
possibility that increasing the number of people who can be
diagnosed with some form of mental illness, however mild, will
effectively expand the market for psychiatric
medications. At the very least, these affiliations might
have biased the Manual developers toward biological diagnoses
and treatments. At the worst, it raises the possibility
that Big Pharma might encourage clinicians to formulate new
diagnoses that expand the market for available psychotropic
drugs -- what Marcia Angell, the former editor of the New
England Journal of Medicine, has called a
"patent-extending game" (see her book, the Truth About
Drug Companies: How They Deceive Us and What We Can Do About
It, 2004).
In 1993, the editors of DSM-IV considered, but
rejected, a proposal for a new diagnosis of Pre-Menstrual
Dysphoric Disorder (PMDD), a severe form of Premenstrual
Syndrome (PMS) experienced by some women of
childbearing age: previously, it was known as Late
Luteal Phase Dysphoric Disorder (LLPDD). At
roughly the same time, SmithKline, a major pharmaceutical
company, was losing its patent on Prozac, a drug used in
the treatment of depression; SmithKline repackaged Prozac
as Serafem (changing little more than the color of the
pill), and began recommending the "new" drug for the
treatment of this "new" disorder. PMDD was given
official recognition in DSM-5. Many
commentators entertain the suspicion that PMDD was
proposed as part of a strategy to legitimize extending the
patent on Prozac.
Aricept is a drug commonly prescribed for symptom relief
in cases of mild to moderate Alzheimer's Disease
(AD): it doesn't reverse, or even slow, the progression of
the disease, but it does provide temporary relief from
some symptoms. In 1999, some researchers began to
talk about Mild Cognitive Impairment (MCI) as a
"prodromal" or incipient phase of Alzheimer's
disease. Diagnosis of MCI requires objective
evidence of memory impairment -- worse than normal
cognitive aging, but not as severe as AD. But in
2013, some researchers began touting a new syndrome of Subjective
Memory Impairment (SMI)to cover cases where
the patient (or his family) complains about memory
impairment, but does not perform poorly on objective
memory tests. Obviously (just think about the normal
bell-shaped curve for a moment) there are more people with
MCI than with AD, and probably more people with SMI than
MCI -- thus potentially expanding the clientele for drugs
like Aricept.
If college students take Ritalin as a "smart drug",
why shouldn't their grandparents take Aricept for the
same purpose?
Other commentators worry that many DSM-5
diagnoses simply lack validity to begin with. In an
important early paper, Robins and Guze (1970) outlined the
criteria for establishing the validity of any diagnostic
category:
Distinguish the target diagnosis (e.g., schizophrenia)
from other possible diagnoses (e.g., bipolar disorder).
Predict performance on laboratory tests involving
psychological and biological variables.
Correlate with family history of mental disorders.
Predicts the course of the illness.
Predicts the outcome of treatment.
By these standards, more than 40 years
later, many DSM diagnoses do not fare too well.
For example, the American Psychiatric Association proposed to
"field-test" DSM-5 before its actual publication, to
make sure that clinicians could use it reliably to make
diagnoses. Unfortunately, DSM-5 failed its field
trials, in that the rate of disagreement between two
clinicians, applying the same criteria to the same patient,
was unacceptably high.
This state of affairs has led some
investigators to propose alternatives to the DSM.
Some theorists have proposed that diagnosis move from a
categorical structure to a dimensional structure. In
such a system, patients would be assessed along continuous
dimensions representing various aspects of cognition,
emotion, motivation, and behavior -- much as personality
assessment is guided by the Big Five dimensions of
personality.Of course, the precise nature of these
dimensions is something for future research to establish.
Other theorists have proposed moving toward a biological
classification -- perhaps in terms of neurotransmitter
activity. This assumes that all mental illnesses
involve underlying biological abnormalities -- an
assumption which isn't self-evidently true. Some
mental illnesses, such as phobias and certain types of
depression, may reflect maladaptive social learning by
patients whose neural functioning is essentially normal.
Other theorists, including yours truly, have proposed
that the diagnostic categories be based on the results of
laboratory tests -- but laboratory tests of psychopathology,
not of pathological anatomy and physiology. What
these tests might look like is foreshadowed in the next
section, on Experimental Psychopathology.
For now, though, DSM-5 is what
we've got. The Social Security administration won't pay
disability benefits, insurance companies won't pay for
treatment, and courts won't consider the insanity defense, in
the absence of an official psychiatric diagnosis, and DSM
is how psychiatrists officially diagnose patients. It's
as simple as that.
Research Domain Criteria
One
possible alternative diagnostic system, embraced by the
National Institute of Mental Health, is the Research
Domain Criteria (RDoC). Instead of employing
traditional diagnostic categories, such as schizophrenia and
bipolar disorder, RDoC classifies mental processes into
several domains, constructs, and sub-constructs, with each
construct and sub-construct hypothetically linked to a
different neural circuit in the brain.
For example, negative emotionality includes fear, which
is linked to the amygdala.
Frustrative Nonreward (i.e., frustration due to the
withholding of reinforcement for previously reinforced
behaviors)
Positive Valence Systems
Approach Motivation
Reward Valuation
Effort Valuation/Willingness to Work
Expectancy/Reward Prediction Error
Action Selection/Preference-Based Decision Making
Initial Responsiveness to Reward
Sustained Responsiveness to Reward
Reward Learning
Habit
Cognitive Systems
Attention
Perception
Visual Perception
Auditory Perception
Olfactory/Somatosensory/Multimodal Perception
Declarative Memory
Language Behavior
Cognitive (Effortful) Control
Goal Selection
Updating
Representation and Maintenance
Response Selection, Inhibition or Suppression
Working Memory
Active Maintenance
Flexible Updating
Limited Capacity
Interference Control
Systems for Social Processes
Affiliation and Attachment
Attachment Formation and Maintenance
Social Communication
Reception of Facial Communication
Production of Facial Communication
Reception of Non-Facial Communication
Production of Non-Facial Communication
Perception and Understanding of Self
Agency
Self-Knowledge
Perception and Understanding of Others
Animacy Perception
Action Perception
Understanding Mental States
Arousal and Regulatory Systems
Arousal
Circadian Rhythms
Sleep and Wakefulness
Following the medical model, it's
important to get beyond surface symptoms and signs to
underlying pathology. DSM-5 doesn't do that,
it's diagnoses are solely based on signs and symptoms.
Diagnosis in the rest of medicine is of diseases, and
the RDoC is a step in this direction. At the same time,
we can worry about the underlying assumption, which is that
each element of underlying pathology is linked to a
dysfunction in some brain circuit (Insel, "Faulty Circuits", Scientific
American, April 2010). It's not at all clear that
a faulty brain circuit must be involved in every instance of
mental illness. Moreover, the identification of such
circuits is years, decades, maybe centuries away. The
whole project of identifying the circuits of the brain, which
is the raison d'etre of the Human
Connectome Project announced by President Obama in
2013, begins with extremely simple nervous systems, such as aplysia
(the sea slug studied by Eric Kandel and others), and then
move up to the mouse, and only later to the human -- at which
point the process of linking neural circuits to the various
domains can begin. Not in my lifetime, nor yours.
In the meantime, diagnosis needs to
move beyond signs and symptoms to the identification of
underlying pathology through laboratory tests -- underlying psychopathology.
For now, though, and for the foreseeable
future, psychiatric diagnosis is going to be based on symptoms
and signs, and organized by something very much like DSM-5.
This line of research in experimental psychopathology
has a long and distinguished history, going back to Emil
Kraepelin's studies of schizophrenia using Donders's
reaction-time methodology. While the RDoC claims to be
"agnostic" about the traditional diagnostic categories
(actually, far from being agnostic, it rejects them),
experimental psychopathology takes them as a starting point,
and tries to identify the pathological mental processes that
underlie them. One result of this work should be the
more fine-grained classification, moving beyond superficial
symptoms and signs, that the RDoC seeks -- but without the
excessive biologizing.
For critiques of psychiatric
diagnosis and DSM, see:
The Selling of DSM (1992) and Making
Us Crazy (1997) by Herb Kutchins.
They Say You're Crazy (1996) by Paula
Caplan.
"The Epidemic of Mental Illness: Why?" and "The
Illusions of Psychiatry" an essay-review of
several books critical of psychiatry by Marcia
Angell (New York Review of Books, June 23
and July 14, 2011).
"Head Case: Can Psychiatry Be a Science?" by
Louis Menand (New Yorker, March 1, 2010).
The Book of Woe: The DSM and the Unmaking of
Psychiatry (2013) by Gary Greenberg, who
doesn't seem to like diagnosis at all (he also
wrote another book, entitled Manufacturing
Depression).
Saving Normal: An Insider's Revolt Against
Out-of-Control Psychiatric Diagnosis, DSM-5, Big
Pharma, and the Medicalization of Ordinary Life
(2013) by Allen Frances (who led the task force
that prepared DSM-IV, but thinks that DSM-5
takes an approach to diagnosis that has become
outmoded).
"Three Approaches to Understanding and
Classifying Mental Disorder: ICD-11, DSM-5,
and the National Institute of Mental Health's
Research Domain Criteria (RDoC)" by Lee Ana Clark
et al. (Psychological Science in the Public
Interest, 2017). A comprehensive
overview of contemporary approaches to psychiatric
diagnosis, emphasizing differences between DSM
and RDoC.
Experimental Psychopathology
Current diagnostic practices classify
illness based on surface symptoms, but the symptoms are not
the disease. Rather, symptoms are assumed to be caused by some
underlying disease process --pathology.
Beyond Surface Symptoms to Underlying Pathology
In medicine, symptoms are not the
disease, and progress in medical understanding is marked by a
shift in focus from symptoms to underlying disease processes
-- to underlying pathology revealed by laboratory analyses of
structure and function whose results are interpreted in the
light of a theoretical understanding of normal function.
Consider
the example of fever, manifested by chills (a symptom
about which patients complain) and increased body temperature
(a sign, indicated by a thermometer). Well into the 19th
century the medical nosology included a large number of
different "types" of fever, based on the symptoms accompanying
the fever and the circumstances under which the fever
occurred. In fact, Benjamin Rush, the pioneering American
physician of the Revolutionary War era, thought there was only
one disease -- fever. But nobody diagnoses and
treats fever anymore, because fever is viewed as a symptom of
an underlying bacterial infection. Physicians may try to
reduce a patient's fever, as an emergency measure, but most of
their efforts are devoted to identifying the underlying
infection (through blood tests) and then treating it (through
antibiotics).
In "Rocky Mountain spotted fever" the
patient presents with chills and elevated body
temperature, as well as a petechial rash beginning on
the wrists and ankles; the illness was first diagnosed
in the Rocky Mountain area of the United States.
Initially, treatment focused on bring the fever down
with cold compresses, or else simply letting the fever
"run its course". Now, however, a physician who suspects
that a patient suffers from this disease will order a
laboratory test to look for serum antibodies to the Rickettsia
rickettsii virus, which is transmitted by a wood
tick found in the western United States. Treatment
entails finding the tick and removing it from the
patient's skin, followed by a course of antibiotics to
eliminate the infection. This treatment, applied in a
timely fashion, results in a complete cure, not just
symptom relief. Similarly, efforts at preventing the
disease are aimed at eliminating the tick from the
environment through insecticide sprays.
The Way We Diagnose Now (in the Rest of Medicine)
Lisa Sanders, a physician on the faculty of
the Yale School of Medicine, occasionally contributes a
column to the New York Times Magazine in which she
shows how a puzzling medical diagnosis was resolved through
the interpretation of laboratory tests that went beyond the
usual symptoms, signs, and history. Here are a couple of
examples from her 2003 columns:
A middle-aged man with a history of diabetes,
hypothyroidism, and bone marrow dysfunction leading to
anemia complained of pain in the hips and buttocks and
difficulty walking; he was comfortable so long as his legs
were not bearing weight. An initial diagnosis of sciatica,
based on the patient's symptoms, didn't quite fit. X-rays
were negative, as were blood tests for infection or
destruction of muscle tissue. However, an MRI revealed an
obstruction in an artery leading to his thigh, a
complication of diabetes, that was a condition similar to
a heart attack, including "ischemic" muscle pain
(09/07/03).
A young man with morbid obesity (5'7", 350 pounds) was
admitted to the Intensive Care Unit complaining of
difficulty breathing and extreme fatigue. A test showed
that the oxygen in his blood was only 88% of normal. Blood
tests suggested an infection in the lungs, while X-rays
revealed pneumonia. The patient's obesity was preventing
him from clearing carbon dioxide from his blood, and the
buildup was causing his sleepiness. The disease,
hypoventilation syndrome, is also known as Pickwickian
syndrome, after an obese, chronically sleepy character in
Charles Dickens's Pickwick Papers
(09/21/03).
A plump woman in her 50s was taken to the emergency room
after a fall. She complained of chronic back pain. An
X-ray revealed a collapsed vertebra in her lower spine,
and the mottled appearance of surrounding vertebrae
suggested cancer. In fact, further physical examination,
confirmed by further tests, revealed a cancer which had
metastasized from her breast to her ribs, hips, and spine
(10/19/03).
A young woman with complained of looking like a man, and
being mistaken for male. She presented with a somewhat
"masculine" appearance, including facial hair, bearing,
and voice. Her menstrual periods were irregular. She had
no signs of a hormonal abnormality such as congenital
adrenal hyperplasia (discussed in the lecture supplements
on Psychological Development). Physical examination
revealed male pattern baldness, and patches of darkened
skin often associated with high levels of circulating
insulin. In the absence of a test that could definitively
confirm the diagnosis, the patient was treated with
medication that would improve her response to insulin, and
thus lower her levels of circulating insulin. In response,
the patient lost some weight and regained menstrual
regularity, consonant with the diagnosis. But the patient
was also referred to an endocrinologist for further
laboratory tests of hormonal dysfunction.
A man in his 50s, being treated for high cholesterol but
with no other health problems, complained of shortness of
breath, but no other symptoms. The absence of fever or
cough ruled out pneumonia. Evaluations of cardiovascular
function ruled out heart disease. A course of antibiotics
had no effect, ruling out infection. A bronchoscopy was
negative for both infection or cancer. The pattern of
negative findings led to a diagnosis of interstitial lung
disease by default -- it was the only remaining possible
cause of the patient's symptoms. In fact, a review of the
bronchoscopy results did reveal a white blood cell anomaly
consistent with ILD, which may have been triggered by the
Lipitor the patient was taking to control his cholesterol
levels. The patient's condition improved when he was taken
off the Lipitor and put on anti-inflammatory steroids --
an outcome consistent with the diagnosis of ILD.
These examples illustrate how diagnosis is
done in advanced, scientific medicine:
The patient's symptomatic complaints, and signs revealed
by physical examination, lead the physician to generate a
hypothetical -- that the patient has a particular disease,
which accounts for for the observed signs and symptoms.
This diagnosis is then confirmed or disconfirmed through
laboratory tests.
If the tests are positive, treatment proceeds in
accordance with the confirmed diagnosis.
If the tests are negative, a new hypothesis is
generated, and new tests are performed.
If no definitive tests are available, a diagnosis may be
supported retrospectively through the patient's response
to treatment.
If the patient responds positively, then the diagnosis
is provisionally confirmed.
But if the patient does not respond positively, a new
diagnosis may be hypothesized, and a new treatment
ordered in an attempt to confirm the hypothesis.
In any event, the patient's response to
treatment is assessed by laboratory tests: if the diagnosis
is correct, and the treatment is working, the patient's
scores will improve on the very tests that generated the
diagnosis in the first place.
On occasion, the correlation between symptoms
and disease may be so high that no tests are ordered. But in
most cases, medical diagnosis is based on laboratory tests,
not presenting symptoms, and the success of treatment is
confirmed by laboratory tests as well.
In medicine, pathology affects bodily
functions through lesions in anatomical structures (e.g., a
skull fracture or lung cancer), abnormalities in physiological
functions (e.g., hypertension or sinus arrhythmia), or
infection by micro-organisms (e.g., the influenza virus; in
addition to viral infections, there are also infections by
bacteria, fungi, chlamydiae, rickettsiae, and microplasmas).
Modern medical diagnosis is based on evidence of these
pathological conditions, as revealed by objective laboratory
tests.
There are parallels in the
medical model of psychopathology:
Abnormalities in Mental Structures and Processes,
roughly analogous to the anatomical and physiological
abnormalities in physical medicine. In these cases of psychological
deficit,something has gone wrong with the patient's
basic mental apparatus -- the cognitive, emotional, and
motivational systems governing the person's experience,
thought, and action. Presumably, there is also some
underlying biological abnormality contributing to the
abnormal mental function.
Abnormalities in Mental States (thoughts,
feelings, and desires) constructed by mental structures
and functions (and their biological substrates) that are
essentially intact. These abnormal mental states --
beliefs, expectations, thoughts, feelings, and desires --
are the mental analogies of infections.
In medicine, underlying
pathology is revealed by laboratory analyses interpreted in
the light of our understanding of normal structure and
function. In psychopathology, such laboratory research is
known as experimental psychopathology. Experimental
psychopathology tries to identify the causes of the patient's
manifest symptoms. It is basic research on psychopathology, as
opposed to applied research on diagnosis and treatment, and it
comes in two major forms:
laboratory studies of psychological deficit and
laboratory models of psychopathology.
Attentional Deficits in Schizophrenia
Studies of
psychological deficit in schizophrenia have a long history,
dating back to experimental work by Kraepelin, in Wundt's
laboratory, who used Donders's reaction time technique to
measure the speed of mental processes in patients with
dementia praecox (presenile dementia), the syndrome later
renamed schizophrenia. One highly prominent theory of
schizophrenia holds that the psychological deficit underlying
the patient's presenting symptoms affects the attentional
system. According to this theory, schizophrenics suffer from a
breakdown in selective attention that renders them highly
distractable and unable to filter out irrelevant ideas. The
patient shows thought and language disorder because he cannot
keep track of what he is thinking and saying; he withdraws
socially to shut out this chaos of stimulation. And, in fact,
laboratory tests confirm that patients with schizophrenia have
a number of difficulties with attention.
The
information-processing deficits in schizophrenia appear to
begin at the very beginning of the information-processing
sequence.Think
of the multi-store model discussed in the lectures on
memory.In that
model, stimulus information is briefly held in
modality-specific sensory registers, from which it is
extracted into short-term or working memory for further
processing, and then encoded into long-term memory.Studies of
information-processing in schizophrenia have focused on the
sensory registers, working memory, and attention.If things go wrong
at these earliest stages of information processing, lots of
other things will go wrong as well.
Consider,
for example, a study by Wishner and Wahl (1974) of
dichotic listening in schizophrenia (there are other
studies of this topic, but I chose this one because Wishner
was a teacher of mine in graduate school and Wahl was a
graduate-student colleague).In
this paradigm, different messages are played through earphones
to the two ears, and the subject is instructed to shadow
one message, repeating its words aloud as they are spoken, and
ignore the other. There is little or no impairment when normal
subjects shadow a single message, with no distracting message
coming over the other ear. When the distracting channel is
added, however, subjects begin to make shadowing errors:
omissions of parts of the target message and intrusions of the
irrelevant message, and recall of the target message.Wishner and Wahl found that schizophrenics
were particularly prone to make shadowing errors: more
omissions and more intrusions, especially when the target
message was played at a relatively fast speed;, and poorer
recall of words from the target message, even when no
distractor was present. These results are consistent with the
hypothesis that schizophrenics suffer from an attentional
deficit.
Comparable
findings were obtained in a study of visual attention by
Saccuzzo and Shubert (1981) employing the backward masking
paradigm. In this procedure, an array of digits or letters is
presented very briefly, so that there is not much opportunity
for it to register in a very short-term memory store known as
iconic memory (see the lecture supplements on Memory).
Presentation of this array is followed by a "masking" stimulus
that effectively displaces the array from iconic memory,
preventing it from being further processed in "primary",
"short-term, or "working" memory. Therefore, identification of
the elements in the array requires highly focused attention,
so that the subject can process the information from the array
into primary memory before its representation disappears from
iconic memory. In the experiment, subjects had to search for
the letter T in an array of As, or for the
letter A in an array of Ts: if it is present,
they simply say "yes" and another trial begins.The investigators varied the
"stimulus-onset asynchrony" (SOA), or the interval between the
onset of the array and the onset of the mask -- essentially,
the amount of time that a representation of the array resides
in iconic memory. They found that schizophrenics were
generally poorer at target detection than controls, especially
at longer SOAs. They concluded that it takes longer for
schizophrenics to transfer information from iconic to primary
memory. By virtue of this slower rate of information
processing, schizophrenics miss a lot of what goes on around
them, and are more distractable.
In
recent years, much attention has focused on working memory
in schizophrenia.You’ll
remember from an earlier lecture that working memory enables
an individual to maintain information in an active state,
over short periods of time, while it is being manipulated by
other cognitive processes.This information may be extracted from perception or
retrieved from memory.As such, working memory is critical for a wide
variety of cognitive processes, such as selective attention,
including both focusing on needed information and inhibition
of irrelevant information.A problem in working memory can permeate far into
cognitive function, affecting memory, reasoning,
problem-solving, and language.10
Working memory is often studied with
variants of the Sternberg task, discussed at length in the
lecture on methods and statistics.In the Sternberg
task, a subject is asked to memorize a small set of items, and
then to search that set for a particular target. It’s
different from the Sperling task.In the Sperling
task, subjects have to inspect a study set presented as a
visual array.In
the Sternberg task, they have to hold a representation of the
study set in working memory while they search it.Sternberg’s basic
finding, you’ll remember, was that response latency varied
with the size of the search set, indicating a serial,
self-terminating search process.An experiment by Paul Metzak and his colleagues
compared schizophrenic patients with a group of normal control
subjects who had been matched with the patients on such
demographic variables as age and education.
Like Sternberg, Metzak found that
accuracy decreased, and response latency increased, with the
size of the study set.But this variable had a greater effect on the
performance of the schizophrenic patients than on the normal
subjects.Performance
especially deteriorated at the largest set size.It’s as if the
patients were overwhelmed by the information they had to
process – maybe because they’re processing information so
slowly, as in the Saccuzzo experiments in iconic memory.
Working
memory consists of several different components.First, there are
modality-specific buffers which maintain information in an
active state.These
elements are similar to the traditional concept of
short-term memory, and there appears to be no problem with
them in schizophrenia.Then there is a central executive, which actually
guides various information-processing tasks, manipulating
and transforming information held by the buffers.Here is where the
psychological deficit in schizophrenia appears to be
located.Other
research shows that there is a particular problem with a
component of the central executive that represents and
maintains contextual information that is relevant to current
tasks – information about the task being performed, other
information that has been recently processed, and what’s
coming next.This
central executive appears to be mediated by the dorsolateral
prefrontal cortex.Interestingly,
this region of the brain is part of a system modulated by
dopamine, and the antipsychotic drugs used in the treatment
of schizophrenia are antagonists of this neurotransmitter.
Studies
of dichotic listening, backward masking, and working memory
illuminate schizophrenic deficiencies in central mechanisms of
attention, but attention is also regulated by peripheral
mechanisms -- as when we turn our heads or eyes to shift our
attention from one object to another. Holzman and his
colleagues have studied the peripheral mechanisms of attention
with an eye-tracking paradigm in which subjects are
asked to hold their head in a fixed position and move their
eyes to track a target moving smoothly across a screen; they
then examine the subjects' pursuit eye movements (PEMs) as
they follow the target. Some aspects of these eye movements
are not consciously perceptible to the subject, but can be
recorded by an electrooculogram (EOG) similar to that used in
sleep research, or by special infrared devices.
Holzman et al. have found that in
contrast to the smooth pursuit eye movements (SPEMs)
characteristic of normals, schizophrenics show eye movements
that are more jagged.About
70% of schizophrenic patients show anomalous PEMs, but PEM
anomalies also show up in relatives of patients who are not
themselves diagnosed with schizophrenia.Accordingly, Holzman has
suggested that abnormal PEMs might be a biological marker
for schizophrenia, perhaps indicating an underlying
malfunction in the frontal-lobe of the brain, particularly in
those centers involved in the peripheral control of attention.
Interestingly, Holzman and his colleagues have found that
abnormal PEMs are related to various aspects of thought
disorder, as measured in patients' verbal protocols. However,
abnormal PEMs are associated with thought disorder across a
wide variety of diagnoses, so this aspect of attentional
deficit may not be specific to schizophrenia.
Most
experimental studies of schizophrenia focus on various aspects
of cognitive function, such as attentional deficits, but
schizophrenia can involve problems with emotional function as
well. Consider anhedonia, one of the classic "Four As"
of schizophrenia. Many schizophrenics show flat or bunted
affect, or else affect that is inappropriate to the situation.
But that's their display of affect. Recall Lang's
multiple systems view of attention, according to which
emotional responses have three different components: a
subjective feeling state, overt behavior, and covert
physiological response.
In one
experiment, Kring and Neale (1998) showed emotional (positive
and negative) and neutral films to schizophrenic patients and
controls, and measured all three components of emotional
response. In terms of facial expressions, schizophrenics were,
indeed, less reactive than controls -- in terms of the
frequency, intensity, and duration. But they were actually more
reactive when their covert physiological responses were
measured by a psychophysiological index known as skin
conductance. The self-reported emotional responses of
schizophrenic patients were somewhat muted, compared to
controls, but both patients and controls showed the same
pattern of response to positive and negative films. So,
schizophrenics do not appear to be emotionally
responsive, in terms of their facial expressions. But in terms
of their subjective feeling states, and their physiological
response to emotional stimuli, they appear to be experiencing
emotion -- even if they aren't showing it in their behavior.
Attention-Deficit Disorder
The problem with diagnosing mental
illness based on symptoms is illustrated by attention
deficit hyperactivity disorder (ADHD), which is
typically diagnosed in children based on such symptoms as
failure to pay attention in school or play, running around the
room, climbing on things, fidgeting and squirming, and the
like. But adults with ADHD don't necessarily do these things.
Instead, they display other, more age-appropriate symptoms
such as difficulties in "wrapping up" the final details of a
project, getting and keeping things in order, remembering
appointments, and the like. Both sets of symptoms may have a
common origin in some attentional dysfunction, and perhaps a
common standard for diagnosis, applicable to children and
adults alike, could be achieved by the development of
laboratory tests that assess attentional functions directly.
Laboratory Models of Psychopathology
In addition to studies of
psychological deficit, it is sometimes possible to create
laboratory models of psychopathology, inducing in normal
individuals a syndrome that, in at least some respects,
resembles some form of actual mental illness. Laboratory
models are rarely if ever exact replicas of mental illnesses,
down to the last detail; rather, they usual mimic one or more
characteristic symptoms of some syndrome. In a sense,
laboratory models constitute theories of how symptoms arise in
actual patients, because they are based on the assumption that
the causative agents that effectively produce symptoms in the
lab parallel those that are present in the real world outside
the laboratory. Thus laboratory models can be used to test
proposals concerning the origins, treatment, and prevention of
mental illness. As such, they can be evaluated on a number of
dimensions:
behavioral (i.e., descriptive features of symptoms and
syndromes);
cause;
cure;
prevention; and
underlying biological structures and processes.
Anxiety Disorders
Like studies of psychological deficit,
laboratory models of psychopathology have a history that goes
fairly far back in time -- but this time, to Pavlov's
laboratory rather than Wundt's. In some early studies of
discrimination learning, dogs were conditioned to salivate to
a circle or an ellipse, and then the axes of the stimulus were
progressively changed, so that the circle became more
elliptical, or the ellipse more circular. The result was that,
at some point, the dogs became distressed -- seemingly anxious
-- a phenomenon that became known as experimental neurosis.
One explanation (proposed by Sue Mineka and myself) was that
this increase in anxiety occurred because the animals could no
longer predict the onset of the food US. Unpredictability
causes anxiety (hold this thought, because in a little while
we'll discuss another laboratory model that indicates that
uncontrollability causes depression).
In addition, conditioned
fear has served as a laboratory model of phobia, while
conditioned avoidance has served as a laboratory model for
obsessive-compulsive disorder.
In conditioned fear, the animal becomes afraid of a
previously neutral stimulus that is associated with fear,
such as a tone that predicts shock.
In 1920, John B. Watson (who gave us the doctrines of
behaviorism) and his student Rosalie Rayner showed that
they could condition phobia-like levels of fear of furry
things in an infant, known to us as "Albert B.", or more
colloquially "Little Albert", by making a loud noise
whenever he came into close proximity to an
otherwise-harmless white rat.Link
to a a video of the Little Albert study.
The case was controversial, not just on the obvious
ethical grounds that they were inducing fear in a
child who was not fearful before, but because they
didn't engage in an extinction procedure that would
have eliminated Albert's fear response.
Inevitably, questions are often asked about what
happened to Little Albert. We don't know for
sure, because Watson left academia shortly thereafter
(following an affair with Rayner, which led to his
divorce) -- he turned to a career in advertising with
the firm of J. Walter Thompson, for whom he invented
the concept of the coffee break" as part of a campaign
for Maxwell House. When he died, his wife,
following his instructions, burned all of his papers.
In 2009, "Little Albert" was plausibly identified
as Douglas Merritte, son of a wet nurse at Johns
Hopkins Hospital. A 2012 article also suggests,
based on films of Albert, that he was not exactly
"normal" to begin with: he may have suffered from a
form of hydrocephalus, an accumulation of
cerebrospinal fluid in the brain. Douglas died when
he was six years old, presumably of the consequences
of his neurological condition (Beck et al., 2009;
Fridlund et al., 2012)).
But in 2014, another group of investigators
pointed to another child, William Albert Barger, who
had been born at about the same time as Merritte,
who died in 2007 (Powell et al., 2014)..
But in the absence of any followup documentation,
we'll never know for sure.
In 1958, Joseph Wolpe reported a series of studies
of conditioned fear and its extinction in cats, which
laid the scientific foundation for systematic
desensitization, an early form of behavior
therapy.
Research by Sue Mineka (already described in the
lectures on Learning)
on the acquisition of snake fear in lab-reared rhesus
monkeys showed that conditioned fear could be acquired
vicariously, without direct exposure to the shock, which
offered an explanation for why many phobics report not
having had unpleasant encounters with the objects of
their phobia.
Although in principle we can acquire phobic-like fears
of just about anything, including teddy bears, in
practice the phobias encountered clinically are
restricted to a relatively narrow range of objects:
heights, darkness, being stared at by other people,
things that crawl or slither -- you get the idea. It's
been suggested that, like snake fear in lab-reared
rhesus monkeys, clinical phobias represent highly
prepared fear responses, part of our evolutionary
heritage.
In much the same way, avoidance learning can serve as a
laboratory model of obsessive-compulsive disorder.
Many compulsions -- like constantly checking the door
to see if it is locked -- seem to reflect the patient's
attempt to avoid or prevent some undesirable outcome.
And, of course, the behavior is reinforced by the fact
that the undesirable outcome never occurs. So the
patient continues doing it. Similarly, avoidance
responses are very difficult to extinguish -- precisely
because they succeed so well that the animal never
learns that the shock has been turned off!
For a personal account of OCD, as well as good
coverage of the scientific literature, see the Man Who
Couldn't Stop: OCD and the True Story of a Life Lost in
Thought by David Adam (2015). Adam himself fell
into the clutches of OCD after having unprotected not-quite
sexual intercourse as a college student. He became
obsessed with the idea that he might contract HIV-AIDS, and
went to great lengths to ward off that outcome.
Learned Helplessness and Depression
Of
particular interest is the development of learned
helplessness as a laboratory model of depression. As
discussed earlier (in the lectures on Learning), learned
helplessness was initially observed in studies designed to
test Mowrer's "two-factor" theory of avoidance learning. In
avoidance learning, a conditioned stimulus (such as a tone) is
followed by prolonged shock as an unconditioned stimulus. If
the animal makes a certain conditioned response (such as
moving from one side of the shuttlebox to the other) after the
onset of the US, it can turn the US off; termination of the US
constitutes reinforcement of an escape response. If it makes
the CR after the onset of the CS, but before the onset of the
US, the US is prevented from occurring at all; this reinforces
an avoidance response. Martin Seligman and his colleagues
discovered that prior exposure to inescapable shock interfered
with escape and avoidance learning. In their analysis, prior
experience with inescapable shock taught the animal that shock
was uncontrollable, and this learning generalized to the new
situation of the shuttlebox. The learned helplessness
experiments underscore the principle that in instrumental
conditioning the organism is learning to control its
environment.
The animals in these
experiments learned to be helpless, but Seligman and his
colleagues also observed that they looked and behaved as if
they were "depressed" (if you've ever seen a sad dog, you know
what they meant). This led Seligman to propose that learned
helplessness is a laboratory model for some forms of
depression -- i.e., that some people become depressed by
virtue of a history of uncontrollable aversive events in their
lives.
Subsequent research by
Seligman and others, including Steven Maier, Lyn Abramson, and
Lauren Alloy, identified a number of parallels between learned
helplessness and depression:
Symptoms: depression, like LH, is characterized
by symptoms of passivity, negative expectations, lack of
aggression, and loss of appetite and sexual interest; in
both learned helplessness and depression, these symptoms
dissipate with time.
Cause: some depressives, like animals in the LH
experiments, have histories of life experiences from which
they learned that outcomes were independent of their
behavior.
Cure: depression, like LH, can often be overcome
by treatments that change the patient's beliefs and
expectations (this is what cognitive therapy explicitly
tries to do). Just as electroconvulsive therapy (ECT) can
successfully treat depression, so electroconvulsive shock
(ECS) can alleviate LH. Just as depressed patients respond
to antidepressant drugs, so helpless animals respond
positively to drugs that stimulate the norepinephrine
system.
Prevention: individuals who are relatively
invulnerable to depression often have a life history
characterized by many mastery experiences; similarly,
animals can be "inoculated" against LH by giving them
prior experience with control.
Biological Substrates: animals who have undergone
LH treatments give evidence of norepinephrine depletion.
The
learned helplessness model of depression, as originally
formulated, is not complete, and nobody claims that LH
underlies all forms of depression. But Abramson and Alloy have
suggested that a certain type of depression, which they label
helplessness depression, is caused by the kinds of
experiences modeled in the LH experiments.
Abramson,
Alloy, and their colleagues subsequently modified Seligman's
theory with the hopelessness theory of depression.
They argued that the experience of uncontrollable aversive
events was not enough to make people (or dogs, for that
matter) depressed. Sometimes, people (and dogs) respond to
uncontrollable aversive events with anger, instead.
Abramson and Alloy
proposed that uncontrollability led to depression only when
the individual made a certain causal attribution
concerning the uncontrollability. They argued that the
explanations that people make for various events vary on
certain dimensions:
Internal vs. external -- does responsibility for
the event lie with the person himself, or with some
external agent?
Stable vs. variable -- does the event always work
out that way, or is the outcome sometimes different?
Global vs. local (or specific) -- is it everything
that goes this way, or just some specific thing.
They proposed that uncontrollability
causes depression only when the individual makes an internal,
stable, global attribution for the helplessness -- as if
to say, I can't control this thing, it's my fault that I can't
control it, I can never control this or anything else. If you
thought like this, you'd get depressed, too, and that's the
point.
Abramson and Alloy pointed out that, in
contrast to non-depressed people, depressed people are often
starkly realistic about their inability to control events -- a
characteristic of depressive realism that they
contrasted to the illusion of control that is
characteristic of non-depressed thought. That is,
non-depressed individuals often have an unrealistically
elevated sense of control (which is why many of us think we
can control chance events by picking "lucky" lottery numbers),
while depressed individuals are often quite realistic about
the prospects.
Abramson and Alloy identified this pessimistic
attributional style as a risk factor for what they
called hopelessness depression. They and their
colleagues also constructed a personality questionnaire, the Attributional
Style Questionnaire (ASQ) to identify people who might
be "at risk" for depression, based on this aspect of cognitive
style.
Seligman, for his part, took off from his
studies of helplessness and depression to focus on the other
side of things, and proposed that positive psychology
should focus on the sunny side of life, and the positive
characteristics that enabled people to be resilient in the
face of unpleasant circumstances. In particular, Seligman
has proposed that giving experiences of control to children
who are at risk for depression (by virtue of their
pessimistic attributional style) may help these children
avoid actual episodes of depression.
In the domain of the psychoses,amphetamine
psychosis can serve as a laboratory model of
schizophrenia. High doses of amphetamines, which increase
dopamine activity in the brain, lead to psychological symptoms
similar to those found in acute schizophrenia --
hallucinations, thought disorder, and paranoid delusions. The
behavioral parallels between amphetamine psychosis and
schizophrenia is one source of the dopamine hypothesis of
schizophrenia, discussed below.
Hypnosis and "Hysteria"
While most laboratory
modeling has focused on various anxiety disorders, some
investigators -- again, beginning in the late 19th and early
20th century -- noticed a phenotypic similarity between some
of the phenomena of hypnosis (e.g., suggested blindness,
deafness, and analgesia; suggested paralysis; posthypnotic
amnesia) and some of the characteristic symptoms of
"hysteria", a cluster of syndromes now known as the
dissociative and conversion disorders.
In both hypnosis and "hysteria", pseudoneurological
"symptoms" occur in the absence of brain insult, injury,
or disease.
Both hypnosis and "hysteria" affect explicit,
conscious perception, memory, and action (like conscious
perception or recall), while largely sparing their implicit
counterparts (like priming).
This has suggested that understanding
the mechanisms of hypnosis might help us to understand these
forms of mental illness as well. In fact, it's been proposed
that both the dissociative and conversion disorders result
from a division of consciousness that prevents certain
percepts and memories from being represented in conscious
awareness.
Linking Laboratory Models to Psychological
Deficits
Sometimes,
laboratory models and studies of psychological deficit go
hand-in-hand. Consider experimental research on psychopathy,
or antisocial personality disorder. One feature of psychopathy
is that these individuals tend not to be responsive to
aversive stimulation. On experimental tests, psychopaths often
show a failure of avoidance learning, and they also show a
failure to respond to punishment. Gorenstein and Newman (1980)
observed a similar pattern of behavior in laboratory rats who
had surgical lesions in a subcortical area of the brain known
as the septum. Rats with septal lesions do not freeze
when they are punished, they have difficulty with passive
avoidance learning (i.e., learning not to do something
in order to avoid punishment), and they also have difficulty
with delay of gratification. All of these phenomena, of
course, closely resemble the characteristic symptoms of
psychopathy. This has led to a theory that, by virtue of some
kind of brain disorder, psychopaths, like septal rats, are
unable to suppress habitual behaviors in order in order to
avoid the aversive consequences of these behaviors.
Experimental research by Newman and
others have further clarified the psychological deficit in
psychopathy to problems linking attention to the reward
system. In one experiment, subjects played a
computerized card game: if they turned over a card they would
gain a point if it was a face card, and lose a point if
not. The deck was arranged so that 9 of the first 10
cards were face cards, then 8 of the next ten, 7 of the next
10, and so on, and they could stop whenever they wanted.
Of course, with the deck arranged in this manner, the subjects
began accruing lots of points, and then started losing.
Normal subjects generally stopped playing after about 50
cards, while they were still ahead; but the psychopaths
continued playing, losing everything they had won -- and more.
Newman's latest theory of psychopathy
implicates attention rather than reward per se. The
general idea is that psychopaths have difficulty updating
working memory with new information, once their attention has
been engaged. They can focus attention, but they can't
disengage and shift it very easily.
Still, there does seem to be something
missing in psychopaths' emotional lives. They don't
accurately pick up on other people's facial and vocal
expressions of emotion, especially fear; don't respond
normally to words with positive or negative emotional
connotations.
Returning to Newman's septal rats, Kent
Kiehl (2006) has used fMRI to record brain activity in
psychopaths during various types of tasks. He has found
deficits in a a system of subcortical brain areas known as the
paralimbic system:
the anterior cingulate, which is important for
decision making and other aspects of executive control;
the amygdala, which generates emotional
responses, especially fear;
the orbitofrontal cortex, important for learning
under conditions of reward and punishment;
the posterior cingulate, involved in emotional
processing;
the insula, which mediates perception of pain
and other bodily states;
the temporal pole, involved in the integration
of emotion and perception.
For more on psychopathy, see "Inside the Mind of a
Psychopath" by Kent A. Kiehl and Joshua W. Buckholtz, Scientific
American Mind, September-October 2010.
Linking the Laboratory and the Clinic
We're going to get back to the clinic
in a moment, but the point of this whole exercise is that the
clinical enterprise of understanding and treating mental
illness is not divorced from the sort of basic research that
goes on in university laboratories. We can use various
research paradigms of the sort discussed earlier in this
course -- classical and instrumental conditioning, dichotic
listening, and the like -- to understand the basic mechanisms
by which mental illness occurs -- as well as ways in which we
might more effectively treat mental illness and prevent it
from occurring in the first place.
By virtue of basic laboratory research
we can move beyond the surface signs and symptoms of mental
illness to understand its underlying pathology. And by better
understanding its underlying pathology, we will be able to
formulate better theories of the causes and cure of mental
illness, and better tools for diagnosis, treatment, and
prevention.
In fact, laboratory
research helps us to identify two different ways that mental
illness can occur.
Some forms of psychopathology reflect psychological
deficits -- disruptions affecting basic psychological
functions.
Schizophrenia seems to involve malfunctioning of the
attention system.
Autistic children (and adults) appear to lack a theory
of mind.
Major forms of depression may be caused by a defect in
the system affecting positive or negative affect.
Attention-deficit disorder also, obviously, seems to
involve a malfunctioning of the attention system --
though presumably a different malfunction from the one
implicated in schizophrenia.
Other forms of psychopathology reflect maladaptive
social learning, in the absence of any particular
psychological deficits. The mind is working OK, but the
person has somehow acquired maladaptive knowledge,
expectations, and beliefs.
In phobia, the person has learned to fear and object
that is not, objectively fearsome.
In obsessive-compulsive disorder, the person performs
an avoidance response that isn't, objectively,
necessary.
In hopelessness depression, the person makes
inappropriate causal attributions for unpleasant events.
Some of the psychophysiological disorders appear to
reflect the effects of environmental stress on internal
organs supplied by the autonomic nervous system --
effects that might not occur of the person learned how
to handle stress better.
The Biology of Mental Illness
Where mental illness appears to reflect
maladaptive social learning, we generally assume that the
architecture of the individual's basic mental structures and
processes is largely intact, as are the neural substrates of
that mental architecture. However, where mental illness
appears to reflect an underlying psychological deficit, there
are good reasons to think that the neural substrates of that
mental architecture are malfunctioning as well -- that is,
that the mental disorders are ultimately neurological
disorders. This idea is expressed in Ralph Gerard's old adage
that
The idea that mental illness have
underlying biological causes goes back at least as far as the
19th century -- which is to say, it is almost as old as
scientific medicine and scientific psychology themselves. In
fact, the history of psychiatry and clinical psychology may be
characterized as a cycle in which prevailing views alternate
between "somatogenic" theories that mental illness is due to
biological causes (i.e., brain insult, injury, or disease) and
"psychogenic" theories that mental illness is due to
environmental causes, and that the biology of the nervous
system is no more relevant to mental illness than it is to
normal mental and behavioral functioning.
From Somatogenesis to Psychogenesis and Back
Again
The earliest scientific theories of
mental illness were neurological theories, based on the
assumption, mostly unproven, that patients' symptoms were due
to lesions or infections affecting brain tissue.
With the emergence of Freudian
psychoanalysis, in the late 19th and early 20th centuries, the
predominant theory of mental illness shifted from somatogenic
to psychogenic. Put briefly, Freud and his followers
taught that mental illnesses, particularly the neuroses, had
their origins in conflict and defense. Psychoanalysis,
both Freudian and neo-Freudian, dominated psychiatry well into
the 1950s.
Another important influence on American
psychiatry was Adolph Meyer, who argued that mental patients'
problems had their origins in their life histories, not their
biology.
The pendulum began to shift back toward
somatogenesis in the 1950s, with the introduction of the first
psychotropic ("mind-moving") drugs: Thorazine (1954), a "major
tranquilizer" used in the treatment of schizophrenia; Miltown
(1955), a "minor tranquilizer" used to treat anxiety; and
Marsilid (1957), a "psychic energizer" used in the treatment
of depression. These drugs were discovered more or less
accidentally, but it was soon learned that they (and other
drugs like them) altered the levels of certain
neurotransmitters in the brain. This led to the
hypothesis that schizophrenia, depression, and other forms of
major mental illness were caused by abnormal levels of these
substances.
Let us just note, in passing, that the
logic of this inference is far from airtight. In fact,
it's a variant on the logical error of denying the
antecedent, discussed in the Lecture Supplement on Thinking. The logic
seems to go something like this.
Thorazine relieves the symptoms of schizophrenia.
Thorazine decreases dopamine levels in the brain.
Therefore, schizophrenia must result from excessive
dopamine levels in the brain.
The problem is that the efficacy of a
treatment says nothing about the cause of the illness.
Nobody thinks that a lack of aspirin causes fever to occur.
And, as it happens, the evidence for the
dopamine theory of schizophrenia, and similar theories, is not
completely convincing. There has never been any
convincing demonstration that, prior to treatment,
schizophrenics or depressives actually suffer from any kind of
chemical imbalance in their brains. Still, theories
about chemical imbalances remain very popular.
In fact, over the past 100 years or so,
biological causes have been uncovered for a number of mental
illnesses, whose biological causes were unknown at the time
they were described, and which had previously been attributed
to environmental causes. In this way, some "functional" mental
illnesses have been reclassified as "organic" in nature.
The first of these was a form of dementia associated
with syphilis, a venereal disease, and which is now known
to be caused by infection by the syphilis spirochete, and
which can be cured by timely administration of
antibiotics.
Alzheimer's disease, once labeled as presenile
dementia, is now known to be caused by the build up
of plaques and tangles in brain tissue.
Autism, a developmental disorder once known as Kanner's
syndrome, was once attributed to poor parenting -- and
especially by so-called "refrigerator mothers" (it's
always the mother, isn't it?) who failed to display
emotional warmth toward their children. This was the
theory proposed by Bruno Bettelheim, a prominent
psychoanalyst, and is now known to be completely wrong
(the score is now "Psychoanalysis Zero", while scientific
Psychology is batting much closer to 1000). Kanner
himself, who first described the syndrome in 1943,
believed that it was caused by bad parenting. These
beliefs did not change until autism was diagnosed in the
first child of Bernard Rimland, a biologically oriented
psychologist, and his wife. They knew that they
hadn't been bad parents, not least because their child had
been autistic since birth -- that is, before they had even
had a chance to be bad parents. In 1964, Rimland published
Infantile Autism, a classic monograph on the
subject, in which he proposed that autism had an organic
cause. Although we still do not know what the precise
causes of autism are, we are now quite certain that they
lie not in the environment, or in the patients' childhood
experiences, but presumably reflects malfunctioning in
certain brain systems.
Current Biological Approaches to Mental Illness
According to the dopamine
hypothesis of schizophrenia , the symptoms of
schizophrenia, and their underlying psychopathology, are
caused by excess activity of dopamine, a neurotransmitter
substance. Evidence for the dopamine hypothesis includes:
increased levels of dopamine metabolites in
schizophrenic patients;
the positive effects of antipsychotic medications, many
of which operate to reduce dopamine levels.
In
fact, autopsy studies, and also some brain imaging studies,
indicate that there are increased levels of dopamine
metabolites in schizophrenic patients.And that's
consistent with the dopamine hypothesis.Moreover,
phenothiazine drugs, which are used in the treatment of
schizophrenia, block the neural receptors for dopamine,
impairing the uptake of dopamine by post-synaptic neurons.So the fact that
there are increased levels of dopamine metabolites found in
schizophrenic patients, and that antipsychotic medications
operate to reduce dopamine levels -- these are both factors
that are consistent with the dopamine hypothesis of
schizophrenia.
But
another piece of evidence comes from a laboratory model of
schizophrenia known as amphetamine psychosis.Solomon Snyder and
his colleagues, working at the National Institute of Mental
Health, found that the administration of certain drugs known
as amphetamines can actually produce some of the symptoms of
psychosis, particularly schizophrenia, in rats and other
laboratory animals.They
also noticed that the habitual heavy use of amphetamines by
humans can produce some of the symptoms of schizophrenia as
well -- particularly hallucinations, thought disorder, and
delusions.These
amphetamine drugs, such as Benzedrine (amphetamine),
Dexedrine (dextroamphetamine), and methedrine
(methamphetamine) may cause the user to experience
hallucinations, while habitual, heavy use can cause thought
disorder and paranoid symptoms as well.have
the effect of increasing dopamine activity in the brain.So this laboratory
model -- first studied in rats, then in monkeys, and then in
humans who abuse amphetamine recreationally -- provides
further support for the dopamine hypothesis of
schizophrenia.In these ways, amphetamine psychosis
seems to mimic at least some of the symptoms usually
associated with schizophrenia.
According to the monoamine
hypothesis of depression, the symptoms of depression,
and their underlying psychopathology, are caused by lowered
levels of another class of neurotransmitters, the monoamines,
which include norepinephrine and serotonin. Evidence for the
monoamine hypothesis includes:
decreased levels of monoamine metabolites in depressed
patients;
the positive effects of antipsychotic medications, many
of which operate to increase the levels of monoamines in
the brain; in particular, the selective serotonin reuptake
inhibitors, effectively increase the availability of
serotonin by preventing premature reuptake of the
neurotransmitter by presynaptic neurons.
Is Depression Adaptive?
Depression is so frequent (it has been called
"the common cold of psychiatry"), and has been around for so
long (Robert Burton published The Anatomy of Melancholy
in 1621), that some evolutionary psychologists have
suggested that, counter-intuitively, a tendency toward
depression might actually be an adaptive trait. According to
one argument, the ruminative thinking that is one of the
characteristic symptoms of depression facilitates
problem-solving. The only problem is that depressives
don't solve their problems -- they just stay
depressed.
Actually, that's just one of the problems
with the evolutionary argument. Here are some others:
It's not clear that clinically depressed patients are
all that good at thinking and problem-solving. Most of
the research either involves experimentally manipulated
emotional states, or states of mild depressed mood that
aren't anywhere near clinical severity.
Moreover, the evolutionary argument assumes that
depression is somehow a response to some kind of
instigating psychosocial event -- i.e., whatever problem
the patient is confronting in his or her environment.
But sometimes depression just happens, and it's
difficult or impossible to find an instigating event of
sufficient magnitude to cause such a severe change in
mood.
Even assuming that there is such an event, clinically
significant depression is typically a chronic condition
-- you'd think that, if depression helped people solve
the problems that set their depression off in the first
place, it wouldn't come back so readily.
And finally, a significant proportion of depressed
patients -- not all, or even a majority, but enough --
commit suicide (or attempt it). And suicide is
definitely maladaptive (though I suppose that
evolutionary psychologists could make up a just-so story
about the adaptiveness of suicide, as well!).
This points out the problem with the
adaptationist fallacy that lies at the heart of so many
speculations by evolutionary psychologists. Depression
exists as a human psychological trait, human psychological
traits, like human physical traits, a product of natural
selection; therefore, depression must be adaptive in the
Darwinian sense. A similar argument has been made about
homosexuality (which, of course, isn't a mental illness),
and even about grandmothers (who aren't necessarily mentally
ill either!). But the whole thing begins with a fallacious
assumption, which is that every human trait, whether
biological or psychological, but be adaptive.
It should be understood that these are
only hypotheses about the underlying biology of these
syndromes, and that these hypotheses are surely incomplete.
And sometimes biological hypotheses are
just wrong. In 1998, a paper published in Lancet by
Andrew Wakefield, a British physician, suggested a link
between autism and the childhood vaccine for measles,
mumps, and rubella (MMR). The resulting concern led to a
worldwide reduction in MMR vaccination, as parents hoped to
prevent their children from getting autism. The methodology of
the study was subsequently criticized, and 10 of Wakefield's
12 co-authors subsequently retracted the paper -- as did the
journal in which it was originally published, and Wakefield
lost his license to practice medicine in Britain (he relocated
to the US). In 2011, an investigation published in the British
Medical Journal asserted that Wakefield's paper was not
just methodologically weak but actually fraudulent.In fact,
subsequent, better designed studies show that there is no
evidence for a role of MMR or any other childhood
vaccination in autism. Nevertheless, as of 2011,
Wakefield (who has relocated to the US) continues to assert
such a link, and worldwide MMR vaccination rates have never
returned to their pre-1998 levels -- increasing the risk of
childhood diseases that are entirely preventable.
For an excellent introduction to the
roe of neurotransmitters in mental illness, and the basics
of psychopharmacology, see Drugs and the Brain (Rev.
Ed., 1996) by Solomon Snyder, one of the deans of
psychopharmacology. Because the pharmaceutical
industry is constantly developing new products, the
information on specific drugs is necessarily a little
dated. But the basic ideas haven't changed much, and
neither has the underlying neuroscience. It's a good
place to start..
Etiology of Mental Illness
Somatogenic and psychogenic theories of
mental illness are, first and foremost, theories about the
role of nature and nurture, and we have now learned that the
proper formulation is nature-nurture questions is not "Which
is right?" but rather "How do nature and nurture
interact?". The etiology of mental illness is no
exception.
Genetics of Mental Illness
One place to look for the origins of
psychopathology is in the genes: perhaps certain forms of
mental illness, or at least risk factors for them, are passed
through families through genetic inheritance. We know
that, for many diagnoses, having a family member with mental
illness increases the risk for mental illness in other family
members. Of course, this effect could be environmental
as well as genetic.
The study of the genetic basis of
mental illness began long before Mendel and research on
fruit flies, as the superintendents of 19th-century asylums
for the insane or "feeble-minded" traced the family
histories of their patients, seeking evidence that mental
illness was inherited (and, not incidentally, laying the
intellectual foundations for the pseudoscience of
eugenics). For an historical account of this research,
see Genetics in the Madhouse: The Unknown History of
Human Heredity (2018) by Theodore M. Porter.
The genetic contribution to mental
illness can be assessed by means of the twin-study method
described in the lectures on Psychological Development:
by comparing the similarity of MZ and DZ twins, we can
estimate the contributions of genetics, the shared
environment, and the nonshared environment. When it
comes to personality characteristics, such as the Big Five
personality traits, similarity is measured by means of the
correlation coefficient. In psychiatric genetics,
similarity is more commonly measured by means of the concordance
rate -- that is, the probability that two twins will
have the same psychiatric disorder. The calculations for
heritability differ a little, but the underlying logic is the
same:
If a mental illness is completely inherited, the
concordance rate for MZ twins should be 100%, and for DZ
twins should be 50%.
To the extent that the MZ concordance rate is less than
a perfect 100%, there is a contribution from the nonshared
environment.
This table reflects our best understanding
of the heritability of major forms of mental disorder, as of
2012. The heritability coefficients vary widely, from a
low of .37 for Major Depressive Disorder to a high of .80 for
Autism Spectrum Disorder and .81 for Schizophrenia.
Note, however, two points about this table:
There are many forms of mental illness that are not
represented here -- either because they have not been
studied, or because existing research has yielded low
heritability coefficients.
None of the heritability coefficients is a perfect
1.0. Even for autism and schizophrenia, genetics is
not destiny, and there are plenty of families with an
autistic or schizophrenic family member where the rest of
the family has no significant mental illness.
So, as is generally the case, the
origins of mental illness are not to be found in the genotype
alone. Rather, they will have to be found in gene-by-environment
interactions (GxE) of the sort discussed under the
heading of epigenesis in the lectures on Psychological Development.
Still, once researchers have established
a significant level of heritability for a mental illness, it
makes sense to start searching for the genes responsible (for
a review, see Duncan et al., 2014). Before the 21st
century, this was not really possible. We didn't know
enough about the human genome, and we didn't have the
technology. And even with the mapping of the human
genome, and the availability of (relatively) inexpensive
technology, the task is daunting:
There are some 20-25,000 candidate genes -- not to
mention all that "intergenic" and "intronic" regions in
the genome that are not, technically, genes.
To obtain reliable results, researchers typically need
huge sample sizes.
Until recently, researchers had to
propose, on the basis of some theory, what genes to look
for. So, for example, if they were interested in
schizophrenia, they might look at genes that are involved in
the production and metabolism of the neurotransmitter
dopamine; for depression, they might look for genes involved
with the production and metabolism of the neurotransmitters
norepinephrine or serotonin. This is known as the candidate
gene strategy. However, advances in technology
have permitted researchers to go on "fishing expeditions" in
which they cast their nets more widely, over thousands or
millions of candidate genes and their variants, in what are
known as genome-wide association studies (GWAS).
These studies have begun to yield results -- and,
interestingly, they have been turning up evidence of genes
involved in mental illness other than those "candidates"
hypothesized by various biochemical theories of mental
illness!
It's pretty clear that the search for
"the gene" that is "for" schizophrenia, or any other form of
mental illness, is going to be complicated (Duncan et al.,
2014).
In the first place, there's almost certainly no such
single gene, not for any form of mental illness.
Instead the genetic contribution is more likely to be polygenic
in nature, consist of the accumulation of many different
genes.
For example, there are at least 40 different genetic
loci associated with height.
A recent GWAS identified more than 100 different
genetic loci, and more than 8,000 genetic variants on
these loci, associated with increased risk for
schizophrenia
And these genes, themselves, are not "for" mental
illness in any sense. Any single gene will have
different effects, depending on its local (physical)
environment.
For example, one of the gene loci associated with
schizophrenia also plays a role in the auto-immune
system.
Genetic influences may be pleitropic, meaning
that a single genetic variant may have more than one
phenotypic effect.
For example, some genetic loci are associated with
both schizophrenia and bipolar disorder, suggesting that
they may well be risk factors for major mental illness
(or psychotic disorders) generally.
Some genetic factors may be rare variants,
present in only a very small number of individuals.
And then there is the problem of missing
heritability -- that is, the difference between the
proportion of variance in some phenotype (such as
schizophrenia) that is explained by heritability, and the
proportion explained by specific genetic variants.
For example, we know that approximately 80% of
population variability in height is accounted for by
genetic factors; but the specific genetic loci "for"
height discovered so far account for only 5% of
population variance -- leaving 75% of genetic
variance unexplained.
And finally, there are the problems of epigenetics
discussed in the lectures on Psychological
Development.
Once we've determined that there is, in
fact, a genetic contribution to some mental illness, the next
step is to determine what genes are involved. I say
"genes", plural, because it's clear that there's no single
gene "for" schizophrenia, like the gene for blue or brown eyes
presented in standard elementary accounts of Mendelian
genetics. Rather, much as with intelligence, the genetic
basis for schizophrenia is most likely to involve the
cumulative effects of many genes -- dozens, perhaps hundreds.
Recent advances in understanding the
genetics of schizophrenia offer interesting insights into the
genetic contribution to mental illness more generally.
These advances have been made possible by the Human Genome
Project, which in 2003 delivered a map of the human genome,
indicating the location of each of our roughly 22,500 genes on
our 23 chromosome pairs. Then began the process of
determining the function of each of these genes. Over
the years, gene-mapping has become less expensive and
time-consuming, so it is now possible to search the genomes of
large numbers of individuals for genes that are associated
with various illnesses, employing such techniques candidate
gene association, common variant association,
and copy number variation.
This isn't a course in genetics, and
if you want details of each of these methods, there's an
excellent, highly accessible account of this work in "Runs
in the Family" by Siddhartha Mukherjee (New Yorker,
03/28/2016), and a more technical survey in "Genome-Scale
Neurogenetics Methodology and Meaning" by McCarroll, Feng,
and Hyman (Nature Neuroscience, 2014). This
discussion is largely drawn from these sources.
With data
available on a very large number of individuals, investigators
are able to identify associations between schizophrenia (and
other forms of major mental illness, such as bipolar disorder
and autism) with various portions of the human genome.
This task has been undertaking by a group known as the
Psychiatric Genomics Consortium (PGC). The "Manhattan
plot" at left (so named because it looks like the New York
City Skyline), taken from one such study involving more almost
37,000 patients and more than 110,000 controls, sampled from
20 countries, shows which specific locus on each chromosome is
significantly associated with schizophrenia (Sekar et al., Nature
2016). Of course, with 22,500 genes, a number of
these associations could appear just by chance, so the
investigators employed appropriate statistical corrections.
As expected, based on the hypothesis of polygenic
inheritance, there were lots of such segments -- more than
100, in fact.
Some of these gene loci are known to be associated with
certain neurotransmitters, and others were associated with
axonal transmission and other activity within individual
neurons. Presumably, particular alleles of these genes
predispose the individual to schizophrenia (or bipolar
disorder, or autism, etc.) -- and as more of these alleles
accumulate in the individual's genome, his or her risk for
major mental illness increases.
These sorts of findings would be
expected if, as most theorists believe, major mental illness
is fundamentally a disorder of the central nervous system. But
other findings were more surprising. For example, the
strongest association (the tallest "skyscraper" in the
Manhattan plot above) was on Chromosome 6, in a region known
as the major histocompatibility complex (MHC), whose genes are
linked to the immune system. But how do we get from
the immune system to schizophrenia? Here's one
prominent theory (Sekar et al., Nature, 2016).
The immune system protects the body against disease by
detecting and attacking various pathogens in the body.
The genes in question control what are known as complement
components (CCs), which identify various viruses,
bacteria, and the like for destruction by immune
cells. However, CCs also identify synapses for
destruction. But why would anyone want to destroy
synapses?
Actually, this is a major feature of neural
development. During the course of fetal development,
brain activity creates large numbers of synaptic
connections, ready for use when the newborn infant
encounters the world. During learning, neurons that
fire close together in space and time (remember long
term potentiation?) strengthen their synaptic
connections; other, unused synaptic connections are lost, in
a process known as pruning (as in pruning trees and
bushes). This pruning process, which goes on for about
the first 30 years of life, is a normal process of neural
development and plasticity. The same CCs that identify
pathogens for destruction also identify synapses for
pruning.
A gene in the MHC region of Chromosome 6, known as C4,
comes in two forms, known as C4A and C4B, and individuals
vary in terms of how many C4A and C4B genes they have, and
in what combinations. C4A and C4B generate
corresponding proteins.
A particular variant on C4 elevates the risk for
schizophrenia from 1% to 1.27%. Yes, you read that
right. An elevation of 27%, which sounds like a lot,
but in absolute terms still a very small risk. So C4
alone is not by any means the solution to the genetics of
schizophrenia.
About 27% of the schizophrenic patients in the PGC study
had this variant on C4. But so did 22% of the normal
controls!
Mice that lack the C4 gene under-prune their
synapses.
And it is known that the brains of schizophrenic patients
contain fewer synapses than those of normal controls.
A certain combination of C4 alleles promoting excessive
C4A activity,
This overactivity in the CC system identifies too many
synapses for pruning.
Over-pruning of synapses results in the difficulties in
attention and thinking that are characteristic of
schizophrenia.
The normal process of synapse-pruning begins at birth and
continues for 20-30 years. Thus, in theory,
over-pruning of synapses results in the typical onset of
schizophrenia in late adolescence or the patient's 20s and
30s (schizophrenia used to be called dementia praecox,
or "early dementia").
Understand: I'm not saying that this
theory is the neuroimmunological cue to the secret of the
origins of schizophrenia. It might very well be wrong --
just like most past hypotheses concerning the genetic origins
of schizophrenia.
Another multinational group of
researchers, known as the Brainstorm Consortium performed a
GWAS of 25 different neurological and psychiatric disorders,
involving more than 250,000 patients and more than 750,000
healthy controls -- thanks mostly to European countries whose
national health systems maintain large databases (Anttila et
al. Science, 2018; see also Gandal et al., Science,
2018). As had proved to be the case in previous,
smaller-scale studies, the psychiatric syndromes showed
substantial genetic overlap (the only exception was
post-traumatic stress disorder, which by definition has a
substantial environmental cause). That is to say, a
number of genetic markers were identified for each syndrome,
but the same makers tended to appear from one syndrome to
another. By contrast, the 15 neurological syndromes
studied, including Alzheimer's disease and Parkinson's
disease, showed much more distinct genetic profiles. And there
was little overlap between the psychiatric conditions and the
neurological ones. What to make of this isn't
clear. One possibility is that there is a genetic
component to risk for mental illness in general, and other
factors, whether biological or environmental, determine which
specific mental illness a person will suffer. Another
possibility is that the GWAS method, and genetics in general,
isn't going to tell us much about the etiology of mental
illness.
At the same time, other researchers have
turned their attention to the environment, and in particular
to those features of the environment that interact with one's
genetic heritage.
For more on the search for the genetic basis of
schizophrenia, including a plea that researchers spend more
time searching for environmental factors that might interact
with genetic predispositions, see "Schizophrenia's Unyielding
Mysteries" by Michael Balter, Scientific American,
05/2017.
The Diathesis-Stress Model
The
origins psychopathology (etiology) may be viewed within the
framework of the diathesis-stress model of psychopathology
proposed initially by Meehl (1962) and Rosenthal (1963), and
elaborated more recently by Monroe and Simons (1991) and
Belsky and Pleuss (2009). According to the model:
Diathesis represents a predisposition toward a
specific breakdown in normal mental functioning. Its
source may lie in the person's biological (genetic
-biochemical) endowment, experiential history of social
learning, or both. The diathesis renders the person
vulnerable to, or at risk for, some specific form of
psychopathology (not psychopathology in general). Every
person achieves a more or less successful adaptation to
this genetic or psychosocial "inheritance".
Stress refers to any event (or series of events)
which challenges the person's current level of adaptation
to the diathesis. Again, stress factors may be either
biological or psychosocial in nature.
The interaction of diathesis and stress precipitates an
acute episode of mental illness -- what used to be
called a "nervous breakdown".
Looking backward from the acute episode, we can examine
the patient's level of premorbid adjustment, or
what is sometimes called premorbid personality. In
medicine, the term "premorbid" refers to the patient's
status before he or she became ill.
Individuals with good premorbid personality have
"inherited" relatively little diathesis, whether through
genes or social learning, or made a relatively
successful adjustment to a relatively high level of
diathesis.
Individuals with poor premorbid personality have
"inherited" a relatively high amount of diathesis, or
made a relatively unsuccessful adjustment to a
relatively low level of diathesis.
The diathesis-stress model of
psychopathology is a special case of the person-by-situation
interaction, where diathesis is an attribute of the
person and stress is an attribute of the environment.
In principle, diathesis and stress
factors could combine in a number of ways.
In an additive
model, diathesis and stress are independent of each other, and
the likelihood of an acute episode is simply a function of the
sum of diathesis and stress factors. Following Lewin, we might
symbolize this situation as E =f(D + S).
In a multiplicative
model, diathesis and stress truly interact, so that the
combination is truly potent: following Lewin, it would be
expressed as D =f(D x S).
For individuals carrying substantial levels of
diathesis, relatively little stress would be required to
precipitate an acute episode of mental illness, and the
individual would likely show relatively poor premorbid
adjustment.
On the other hand, catastrophic levels of stress would
likely produce an acute episode even in individuals who
carry little or no pre-existing diathesis, and who would
show relatively good premorbid adjustment.
If diathesis levels are within normal limits, an acute
episode would occur as a function of stressors in the
individual's life.
If stressors are within normal limits, an acute episode
would occur as a function of the individual's level of
diathesis.
Note that diathesis factors are
specific to particular forms of mental illness. In theory,
some particular diathesis predisposes an individual to
schizophrenia, but other specific diathesis would be relevant
to depressive disorder, anxiety disorder, etc. In this way, if
stress precipitates an acute episode of mental illness, that
illness will take a specific form.
Diathesis and Stress in Theory and Practice
Schizophrenia. The diathesis-stress
approach was first articulated in the context of schizophrenia.
With respect to diathesis, there is a clear genetic component
to schizophrenia. Compared to a base rate of about 1% in the
population at large, the concordance rate for schizophrenia is
clearly elevated among relatives. In monozygotic twins, the
concordance rate is about 38%; for dizygotic twins, 8%. Risk
for schizophrenia is also increased if a first-degree relative
(father, mother, brother, sister) is schizophrenic. Among
adoptees, risk is increased if one's biological parent has
schizophrenia, but not if one's adoptive parent has
schizophrenia. These figures are consistent with the
proposition that people can inherit a predisposition to
schizophrenia. But note that the concordance rate is far from
a perfect 100% (in fact, it appears to be far from even 50%),
suggesting that genes are not solely determinative . Any
difference between monozygotic twins must be due to the
unshared environment, and that is where differences in stress
probably come into play. In any event, schizophrenia appears
to occur as the product of the combination is of a shared
genetic diathesis and an unshared environmental stress.
Rosenthal
(1963) originally got his idea about diathesis and stress from
the Genain Quadruplets -- identical quadruplet girls, born in
1930 into a family with a history of mental illness, three of
whom were hospitalized for schizophrenia on at lest one
occasion. "Genain" is a pseudonym, derived from the Greek
words for "dire birth", intended to protect the identity of
the girls and their family. Because they were studied
intensively at the National Institute of Mental Health, they
are known as Nora, Iris, Myra, and Hester. What was
particularly interesting about the twins was that not all of
them fell ill -- at least, Myra was never actually
hospitalized. Thus, schizophrenia is not purely a result of
genetics -- or else, these identical twins would all have had
identical outcomes. Instead, Rosenthal hypothesized that a
genetic diathesis interacted with some environmental stress to
precipitate schizophrenia in some of the children, but not in
all.
Another family challenged by mental
illness were the Galvins -- Mimi, Don, and their 12
children, six of whom -- all boys born between 1945 and 1965
-- ended up with a diagnosis of schizophrenia. The
whole sad story is told by Robert Kolker, a journalist, in Hidden
Valley Road (2020). The post-World War II
interval was the heyday of psychoanalysis, with its theory
that the illness was caused by cold, domineering
"schizophrenogenic" mothers who themselves suffered from a
"perversion of the maternal instinct". An entirely
bogus theory, like the rest of psychoanalysis, but that
didn't prevent Mimi from shouldering the blame; nor did it
prevent the boys from getting treatment that might actually
have helped them. Then came the pharmacological
revolution, and the boys were so filled with antipsychotic
medication that they suffered massive side-effects.
The other six siblings -- four boys and two girls -- escaped
the illness, but not really -- because they grew up in an
often chaotic household (on Hidden Valley Road) that the
parents could barely hold together. What results, in
Kolker's hands, is a compelling depiction of what severe
mental illness can do to a family. And another picture
of the complexities of diathesis-stress theory.
Wherever the boys schizophrenia came from, the presence of
six mentally ill children in a single family can't help but
have piled on the stressors.
One environmental stressor that has
been implicated in schizophrenia is socioeconomic status:
schizophrenia is rare, affecting less than 1% of the
population, but it is more likely to be observed in
individuals with relatively low socioeconomic status. One
theory is that the stresses of lower-class living interact
with a genetic diathesis for schizophrenia, resulting in the
higher incidence -- an idea known as sociogenesis.
However, careful epidemiological studies have shown that low
SES follows, rather than precedes, the onset
of schizophrenia. That is, schizophrenia occurs in all
socioeconomic strata, but when it happens to upper-class
individuals, they tend to drift down to lower socioeconomic
strata -- a phenomenon known as social drift.
However, the failure of the sociogenic
hypothesis does not rule out environmental contributions to
schizophrenia. Other environmental influences that have been
causally linked to schizophrenia include:
Coping failures, including losses and
frustrations of various sorts. Loss, frustration, and
coping failure do not by themselves cause schizophrenia,
but they appear to be the sorts of things that can
precipitate an episode of schizophrenia in someone who is
at risk for it.
Expressed emotion: Schizophrenics who have
recovered from an episode of the illness, and then are
discharged into a home environment in which criticism and
other negative affect is directed at them, or family
members and others become overly emotionally involved with
the patient, are more likely to relapse, and have another
episode.
Lack of Social Support: Schizophrenia is often
associated with a poor prognosis, and the expectation that
schizophrenia is a chronic disease from which patients
never recover. But it turns out that it's possible
for schizophrenics to make a pretty good re-entry into
ordinary, everyday life -- especially if they had made a
good premorbid adjustment before their initial
episode. One key to this recovery is medication, for
symptom control. But another key, equally important,
is social support. If schizophrenic patients learn
to cope with their residual symptoms, and they receive the
support and encouragement of family, friends, neighbors,
and coworkers, the prognosis for successful recovery is
actually pretty good (think about John Nash, subject of A
Beautiful Mind by Silvia Nasr, who won the Nobel
Prize in Economics). If social support can lead to
successful recovery, the implication is that social
support might have prevented the initial episode in the
first place.
One environmental stressor that has
received a great deal of research attention is deviant
communication: Vague and fragmented verbal exchanges,
especially on the part of family members. A longitudinal
research project known as the Finnish Adoptive Family Study of
Schizophrenia examined the long-term outcome of "high risk"
children who were born to 167 women hospitalized for
schizophrenia and control children born 202 women hospitalized
for other illnesses. On medical advice, the children of these
women were given up for adoption. In one study, Wahlberg,
Wynn, and their colleagues tested the adoptive families for
signs of communication deviance, and then tested the adopted
children themselves (known in medical terminology as
"probands", because their family history gives them an
elevated probability of becoming ill) on an index of thought
disorder characteristic of schizophrenia.
When there was little communication deviance in the
adoptive family, the high-risk probands of the
schizophrenic women showed little evidence of thought
disorder.
But with increased levels of communication deviance in
the adoptive family, the incidence of thought disorder in
the schizophrenic probands progressively increased -- but
no such increase was seen in the non-schizophrenic
probands.
This is exactly the kind of
person-environment interaction anticipated by the
diathesis-stress model: the combination of high genetic risk
(being the child of a schizophrenic mother)and high
environmental stress (being exposed to communication deviance
in one's adoptive family) leads to increased occurrence of
schizophrenic symptoms. No such trend occurred, however, in
children who were not already at risk for
schizophrenia.
Now look carefully at the graph. Note that
the level of communication deviance in the adoptive families
of control children "maxes out" at 8 units, while the level
observed in the adoptive families of the high-risk probands
goes as high as 10 units. Perhaps, by some stroke of bad
luck, these high-risk probands were adopted into families
who were carrying more than their fair share of
schizophrenic diathesis. More likely, the high-risk probands
contributed to the high levels of communication deviance
observed in their adoptive families -- communication
deviance that might not have been present, but for the
probands themselves. Perhaps this is another instance of the
person creating the environment to which s/he responds.
Mood Disorder. Studies of
bipolar and (especially) unipolar affective disorder show the
same patterns: clear evidence for a genetic diathesis, but
equally clear evidence for an unshared environmental stress
(we cannot calculate the contributions of genetics, shared
environment, and nonshared environment from concordance rates
in exactly the same way you can for twin correlations, but the
logic is the same).
Ulcers. The diathesis-stress
approach is also relevant to psychosomatic ulcers,
where lesions in the lining of the gastrointestinal system
(that's what peptic ulcers are) occur to people who are under
a high amount of stress.
Gastric ulcers affect the lining of the stomach.
Duodenal ulcers affect the lining of the small intestine
(or duodenum).
There are also esophageal ulcers, which don't concern us
here.
The psychosomatic nature of peptic
ulcers has recently been discounted by some physicians, who
note the presence of a particular bacterial infection,helicobacter
pylori, in the stomachs and small intestines of as many
as 80% of ulcer patients. But while almost everyone who
suffers from ulcers is infected with h. pylori, not
everyone infected with h. pylori has ulcers. In fact,h.
pylori is also found in the gastrointestinal systems of
70% of patients who do not have ulcers! What makes the
difference? Plausibly, stress. Part of the stress response is
to secrete acid into the stomach (to aid in the digestion
process; when it doesn't encounter food, it eats away at the
stomach lining, creating ulcers (gastric ulcers are lesions in
the stomach; duodenal ulcers are lesions in the small
intestine). Infection by h. pylori increases the
gastrointestinal system's vulnerability to ulceration: it is a
genuine diathesis factor. But, prolonged stress-related
autonomic activation (see the discussion of Selye's general
activation syndrome in the lecture supplements on the
Biological Basis of Mind and Behavior) can interact with the
bacteria to make ulcers even more likely to occur.
The diathesis-stress hypothesis is
supported by a laboratory model of ulcers developed by Steven
Maier (one of the investigators involved in the discovery of
learned helplessness). In this model, rats are infected with h.
pylori bacteria, and then are exposed to stress in the
form of unpredictable and uncontrollable shock. This
combination is particularly likely to produce ulcers, compared
to conditions in which neither diathesis nor stress, or only
one factor but not the other, are present.
Phobias. In experimental
psychopathology, phobias are a classical example of
psychopathology acquired through learning -- particularly,
fear conditioning. As such, phobias would seem to be a case of
all stress and no diathesis: the stress is the anxiety that
accompanies exposure to the feared object. So, if a person has
a negative encounter with a snake, he or she will come to fear
snakes. In this conditioning theory of phobia, the snake is a
CS that predicts unpleasant consequences.
This is a fine theory, so far as it
goes, but it has two problems.
One problem is that people with phobias
don't always, or even usually, have histories of negative
experiences with the objects of their fears. Readers who have
phobias concerning snakes, for example, might ask themselves
what snakes have ever done to them. Once in a while a snake
phobic has been bitten by a snake, but not too often. Instead
of resulting from direct experience with the phobic object, it
is more likely that the snake phobia has been acquired through
social learning or vicarious conditioning. That is, people
become afraid of snakes because they know other people who are
afraid of snakes. We learn to fear what other people fear,
without having frightening experiences ourselves.
The second problem is that people don't
always acquire phobias following association of an object with
negative consequences. To use an example from Seligman (the
same theorist who proposed the learned helplessness model of
depression), when we have a bout of food poisoning we don't
become afraid of the crockery and cutlery; we become afraid of
the food. And not just any food we may have eaten; we tend to
become afraid of thinks like Lima beans and cream sauces. In
fact, clinical phobias are largely limited to a relatively
small number of situations: open spaces, high places, the gaze
of other people, and wriggly, slimy things. According to
Seligman, we are prepared by evolution to easily and quickly
acquire conditioned fear responses to these sorts of objects
and situations. In this view, the diathesis in phobia is a set
of "prepared" associations, a part of the organism's
evolutionary heritage, which predispose the individual to
acquire intense fears even with minimal exposure.And the
stress is a negative event. The stressful event can result in
phobic levels of fear, but only by virtue of these prepared
associations.
A
laboratory model of phobias incorporating both social learning
and preparedness has been studied by Mineka and her colleagues
in research described in the lecture supplement on Learning.
Mineka and her colleagues showed that observational learning
was sufficient to produce intense conditioned fear in monkeys
who themselves had no experience of negative consequences in
association with the CS: they learned to fear what other
monkeys feared. But Mineka et al. also found that
observational learning didn't produce fear of just
anything. Through vicarious learning, monkeys acquired
conditioned fear responses to snakes, but not flowers.
According to the preparedness argument, a disposition to fear
snakes is built into monkeys by evolution, and can produce
full-blown snake-fear even in with little or no direct
experience.
The
Dunedin Studies. The interaction of a biological
diathesis with environmental stressors can be illustrated by
two studies by Avshalom Caspi, Terrie Moffitt, and their
associates, based on data collected in the "Dunedin
Multidisciplinary Health and Development Study". In this
project, longitudinal data was collected from a "birth cohort"
of 1,037 children (roughly half of them males) born near
Dunedin, New Zealand, and tested approximately every two or
three years from ages 3 to 26 (actually, they're still being
followed).
In one study,
Caspi et al. (2002) examined the role that the MAOA gene
played in adolescent conduct disorder. This gene, located on
the X chromosome, promotes monoamine oxidase A, a substance
that metabolizes many different neurotransmitters, and which
has been linked to increased aggression in both laboratory
mice and humans. Caspi et al. also explored the role of stress
in conduct disorder -- particularly a history of childhood and
adolescent maltreatment, which some theorists have proposed
initiates an intergenerational "vicious cycle of violence" in
which maltreated boys become maltreating fathers, producing
maltreated boys who also become maltreating fathers. In fact,
subjects with high levels of MAOA activity showed a relatively
low incidence of conduct disorder, regardless of their history
of maltreatment. However, subjects with low levels of MAOA
activity, who also had a history of severe maltreatment,
showed a very high incidence of conduct disorder. The MAOA
gene is a diathesis which interacts with severe maltreatment
to produce conduct disorder.
In another study, Caspi et al. (2003)
examined the role of the 5-HTT gene in major depressive
disorder. This gene, located on chromosome 17q11.2, comes in
two forms, "short" and "long", yielding four genotypes: SS,
SL, LS, or LL. Caspi et al. also explored the role of life
stress in depression, by counting the number of stressful
events occurring in the life of each subject between ages 21
and 26 (in psychology, a "stressful" event can include getting
married as well as getting divorced). Subjects with the LL
form of the genotype showed a relatively low incidence of
depression, regardless of their history of life stress.
However, subjects with the "short" form of the genotype (with
at least one short allele, as in SS, SL, or LS), combined with
a history of many stressful events during the previous five
years, showed a much higher incidence of depression.
Similarly, Fox et al. studied
the role of the 5-HTT gene in pathological shyness --
children and adults who are severely withdrawn. Their study
actually involved multiple assessments of children's
temperament -- how inhibited the children were in the presence
of strangers, and their mothers' ratings of their shyness. The
mothers also provided ratings of the amount of social support
(e.g., friends) their children had. The results of the study
showed a clear gene x environment interaction:
Children with the "short" allele of the 5-HTT gene,
coupled with poor or very poor social support, showed much
higher levels of behavioral inhibition, compared to
children with the "long" allele, or good levels of social
support.
Similarly, children who combined the short allele with
poor social support received much higher ratings of
shyness -- by which, of course, we mean pathological
shyness, not the ordinary sort of shyness that children
(and adults) can display.
Notice the shape of the graphs in the
Fox et al. study of pathological shyness, which combines the
"crossover" and "fan" effects that are so characteristic of
the person-by-situation interaction.
Still another study from the
Caspi-Moffitt group focused on marijuana and psychosis.It’s long been
known that some people who smoked marijuana as adolescents
develop a form of psychosis as adults, but the precise
pathway has been unclear.Certainly, most adolescents who smoke marijuana don’t
develop psychosis, but it does appear to be a risk factor.Caspi and Moffitt
focused their attention on yet another gene, known as COMT,
located on Chromosome 22. COMT is involved in the metabolism
of dopamine, which has been linked to schizophrenia.The gene comes in
two forms, methionine (“Met”), and valine (“Val”).Individuals who
have two copies of the “Met” allele show the fastest
breakdown of dopamine; those with two copies of “Val”, the
slowest; and those with one of each, somewhere in between.So, if you’re a
“MetMet” person, dopamine metabolizes faster, and resides in
your system for less time.Again using subjects from the Dunedin study, Caspi
and Moffitt classified their subjects according to the form
of the COMT gene, and also by their history of adolescent
marijuana use.And when they looked at the
incidence of psychotic symptoms in these subjects when they
were young adults, they found a clear gene-by-environment
interaction.The
affected subjects didn’t always show full-blown schizophrenia
or any other psychotic syndrome.Still, their risk for delusions, hallucinations, and
other “schizophreniform” symptoms was greatly increased if
they had two copies of the “Val” allele, coupled with frequent
marijuana use as adolescents.If they had only one copy of “Val", or two copies of
“Met”, their risk was greatly reduced.
Another study showed how the COMT genotype
interacted with stress to affect performance on a academic
tests (Yeh et al. 2009) -- not, admittedly, a major mental
illness, but perhaps indicative of GxE interactions in anxiety
disorders. Every year, Taiwanese students who wish to
move on from junior to senior high school must take a rigorous
test known as the Basic Competence Test, which measures
educational achievement in a number of subjects, including
Chinese and English language, mathematics, science, social
science, and writing. The BCT is an extremely stressful
"high-stakes" test, because its outcome determines whether the
student will have any chance of going to college (at least in
Taiwan). Yeh drew a sample of 779 Taiwanese high-school
students (i.e., who had already passed the BCT), and examined
their scores on the BCT subtests as a function of their COMT
genotype.
Students with the Met/Met genotype consistently
performed more poorly than those with the Val/Val or
Met/Val genotype.
There were no differences between students with the
Val/Val or Met/Val genotypes.
The conclusion is that having two
copies of the Met genotype renders the person vulnerable to
high levels of stress, to the detriment of performance.
Some of these gene-environment
interactions are controversial.
The specific findings of Caspi and Moffitt, as well as
those of have proved difficult to replicate, possibly
because of the highly unusual population from which they
drew their samples (Duncan et al. 2014).
The interpretation of the gene-by-environment effects
is also subject to controversy.
I have presented them as illustrative of the
diathesis-stress approach, with -- for example -- the
short allele of the 5-HTT gene functioning as a kind of
risk factor, rendering a person more vulnerable to the
effects of a stressful environment.
An alternative view is that the 5-HTT gene, and
presumably others like it, acts as a kind of
"sensitivity gene", amplifying the effects of the
environment.
Possessing the short allele will magnify the
negative effects of exposure to a negative,
stress-filled environment.
But possessing the same short allele will magnify
the positive effects of exposure to a positive,
pleasure-filled environment.
In
particular, the gene-by-environment interaction in
depression, involving the 5-HTT gene, has stimulated a great
deal of interest, but it’s also been controversial.Some researchers
have failed to replicate Caspi and Moffitt’s findings, while
some critics have complained about the assessment of stress.Katja Karg and her
colleagues recently surveyed 56 studies, involving more than
40,000 subjects, and found that, overall, these studies
confirmed the G-by-E effect.A history of stress, especially defined by childhood
maltreatment or life-threatening or chronic medical
conditions, coupled with the “short” form of the 5-HTT gene,
greatly increases one’s risk for a major depressive episode.
So please note that the findings on 5-HTT or COMT, for
example, are not to be taken as firm. Rather, I cite
them here simply as illustrations of a particular approach,
using the diathesis-stress model, that is commonly used to
identify the genetic and environmental contributions
to mental illness. So stay tuned!
The Nature of Diathesis and Stress
In standard presentations of the
diathesis-stress model, the diathesis is often biological
(like the 5-HTT gene) and the stress is often psychosocial
(like stressful life events), but this need not necessarily be
the case.
Usually, we think of biological
diatheses as specific genes, like MAO-A or 5-HTT. But
it's possible that there is a genetic diathesis for a broader
group of mental illnesses. Smoller and his colleagues
(2013) conducted the largest study to date of the genetics of
mental illness, including more than 60,000 subjects from 19
countries (roughly half were patients carrying a psychiatric
diagnosis). They found that five different disorders --
schizophrenia, bipolar disorder, depression, attention deficit
hyperactivity disorder, and autism -- shared a relatively
small set of genetic aberrations in common. For example,
one identical twin might develop schizophrenia, while another
might develop bipolar disorder.
Somewhat similar results were obtained
from another study which extracted RNA (not DNA) from the
cerebral cortex of deceased patients who had been diagnosed
with various forms of major mental illness, such as autism,
schizophrenia, bipolar disorder, depression, and alcoholism
(Gandal et al., Science, 2018). They compared
these assays to samples taken from individuals who did not
carry a psychiatric diagnosis (an obvious control), and from
other patients with a physical illness, irritable bowel
syndrome (in order to control for illness in general).
As in the Smoller study, they found that there was significant
overlap in the patterns of gene expression across the various
syndromes -- except alcoholism, which had a pattern that was
quite distinct compared to the others. For example,
there was considerable overlap in gene activity between
schizophrenia and bipolar disorder -- despite the fact that
the symptoms associated with these two syndromes are very
different.
These studies suggest that there might
be a genetic diathesis for these major forms of mental illness
in general, and that whatever specific mental illness an
affected individual develops would depend on other factors
(perhaps environmental, perhaps genetic as well).
Biological Stressors
In some instances, stress is better
conceptualized as biological rather than psychosocial in
nature.
For example, prenatal and perinatal
complications are often found in the life histories of people
who eventually develop schizophrenia. These are environmental
stressors, but the fact that they occur in the prenatal or
perinatal environment mark them as more biological than
psychosocial in nature. A difficult birth doesn't have the
same meaning for a person as a difficult childhood or
adolescence.
Psychosocial Diatheses
In other instances, diathesis is better
conceptualized as psychosocial rather than biological in
nature
For example, people may be
predisposed to depression by histories of social
learning that lead them to acquire certain beliefs.
Beck has noted the presence of depressogenic
schemata -- what he calls the depressogenic
triad negative views of the self, the world, and the
future -- in the belief systems of many depressed
patients. In Beck's view, these cognitive structures of
knowledge and belief render the person vulnerable to
depression and all its symptoms -- sadness, anhedonia,
guilt, withdrawal, inactivity, and loss of appetite -- in
the face of adverse life events.
Beck has recently expanded his cognitive theory of
depression (Beck & Bredemeier, 2016) to include yet
another diathesis factor: a heightened reactivity to
stress, which causes the individual to view
any loss of "essential human resources" as particularly
"devastating and insurmountable". As a result, it
takes relatively little stress to activate the
depressogenic schemata, leading to the development of
the symptoms of full-blown depression.
Another psychosocial diathesis for depression was
noted by Nolem-Hoeksema (1991; Nolem-Hoeksema et al.,
2008): rumination, as opposed to self-distraction,
perpetuates the symptoms of depression. Especially in
women, a tendency toward rumination may serve some of
the same maladaptive functions as Beck's depressogenic
schemata or Abramson and Alloy's depressogenic
attributional style.
Similarly, Abramson and
Alloy noted that many depressed patients displayed a
particular "depressogenic" attributional (or inferential)
style in which they tended to explain events in
terms of stable, global, internal factors (as opposed to
unstable, local, external ones). In their view, way of
thinking rendered people vulnerable to depression --
because they tend to think that negative events are
uncontrollable even when they aren't. This idea
has led to the hopelessness theory of depression
(Abramson, Metalsky, & Alloy, Psych Rev.,
1989), which states that, in response to negative life
events, individuals with a depressogenic attributional
style will become hopeless, and this persistent state of
hopelessness is the proximal cause of clinical
depression. Note however, that A&A do not
believe that hopelessness lies at the root of all
instances of depression. Instead, they posit that
hopelessness is the cause of a particular subtype of
depression, which they call, naturally enough, hopelessness
depression. This is not as circular as it
sounds. A&A argue that there are many
different forms of major depressive disorder, each with
its own unique etiology, course, prognosis, and
preferred treatment.
There is, of course, an extensive
literature showing that depressed individuals have a
history of negative life experiences.
And there is also an extensive
literature showing that depressed individuals tend
to have a depressogenic attributional style.
It was not until 2018, however,
that A&A, along with their colleagues, put the
whole thing together to show that the depressogenic
attributional style, as a diathesis factor,
interacted with negative life experiences, as a
stress factor, to generate hopelessness, and thus
depression. A study by Mac Giollabhui and her
colleagues, including A&A, tested the
theory with a diverse sample of 249 adolescents,
ages 12–13 years.The subjects were first assessed at baseline
and at subsequent follow-up sessions over
approximately 2.5 years. Employing self-report
questionnaires and clinical interviews, the
investigators assessed attributional style, NLEs,
feelings of hopelessness, depressive symptoms, and
depression diagnosis. Subjects who showed signs of
depression at initial testing were excluded from
further consideration.Statistical analysis indicated that subjects
with a negative attributional style, and a high
number of negative life events displayed more
depressive symptoms, and were more likely to
experience their first acute major depressive
episode within the follow-up period.However,
this was only the case for subjects who also showed
high levels of hopelessness.Subjects
with low levels of hopelessness had fewer symptoms,
and were less likely to experience an episode of
depression.The
study demonstrates the validity of the hopelessness
theory of depression and its clinical relevance in
predicting depression in adolescence.
Consider how this "reversal" of the
standard account of diathesis (psychosocial, not biological)
and stress (biological, not psychosocial) might help explain
the incidence of postpartum depression, which occurs
in some (but not all) women who have recently given birth.
Sudden biochemical changes associated with pregnancy and
childbirth may alter the person's characteristic mood states
and activity levels. These particular alterations may be
similar to those that occur in depression, but they do not
necessarily result in a depressive episode. However, if
these changes are interpreted in terms of Beck's
"depressogenic schemata" or Abramson and Alloy's "depressive
attributional style", they may well be interpreted
in such a manner precipitate an episode of depression. In
this case, the diathesis factor is psychosocial in nature --
a "depressogenic" way of thinking. But mental illness
doesn't occur unless this diathesis interacts with a
stressor-- and in this case, the stressful events are
biochemical in nature, consisting of certain biochemical
changes that occur naturally with pregnancy and parturition.
A similar account could be given of the
depression which occurs in some (but not all) women who are
going through menopause.
Post-traumatic stress disorder
(PTSD) would, at first glance, appear to be an almost "pure"
case of stress-related mental illness. But, in fact, only a
minority of people actually exposed to traumatic levels of
stress actually go on to develop PTSD (there is, of course, an
acute stress disorder affecting large proportions of
trauma victims, but even this isn't universal). This
variability was noted even as far back as World War I, where
it was attributed to individual differences in soldiers'
predisposition to stress. This diathesis might be
biological -- perhaps something related to the functioning of
the hypothalamic-pituitary-adrenal (HPA) axis, or perhaps a
genetic predisposition. Or it might be something
psychological, analogous to the depressogenic schemata and
attributional styles implicated in some forms of
depression. But the basic point is that even in PTSD,
the stressor alone is rarely sufficient to cause the disorder
all by itself; the stressor has to combine with a
predisposition or vulnerability.
Interestingly, the role of diathesis or predisposition in PTSD
has contributed to the reluctance to award honors or
disability benefits to some soldiers suffering from
PTSD. The argument is that the soldiers' disabilities
weren't caused by the stress of war, but rather are related to
personality problems that predated the war -- much as
insurance companies will sometimes deny medical coverage on
grounds of a "pre-existing condition". Setting this
policy issue aside, PTSD may be an example where both
the diathesis and the stress are psychosocial in nature.
Diathesis is often biological, and
stress is often psychosocial, in nature. But the really
important feature of diathesis is that it is something
that the person carries with him into a situation,
either as a biological or a psychosocial "trait". By the same
token, the really important feature of stress is that it is something
that happens to the person in a particular situation,
ether as a biological or psychosocial event (or series of
events).
Treatment of Mental Illness
The diathesis-stress model for the origins of mental illness
offers a framework for understanding their treatment and
prevention as well. So, if mental illness is caused by the
interaction of diathesis and stress, then effective
interventions should alter diathesis factors, stress factors,
or both.
To orient
ourselves, let's first examine what happens during an episode
of mental illness. As in earlier lectures in this
module, we'll be using language derived from medicine patient,symptom, syndrome, and so on, to identify what
we can call, following Steven Hollon, a prominent depression
researcher at Vanderbilt University, and others, the 5 Rs
of Mental Illness. I'll use depression as my
example, but the same general points would apply to any
syndrome of mental illness.
First, let's assume that the patient
begins at a more-or-less "normal" state, with no identifiable
symptoms of mental illness. At some point, however,
given a certain combination of diathesis and stress, he or she
begins to show symptoms of some form of mental illness --
depression, or anxiety disorder, or schizophrenia. At
some point, enough symptoms develop, with enough severity, to
compromise normal functioning, at which point we can say that
the person has "progressed" -- that's the medical term -- to a
full-blown acute episode of mental illness.
Remission. With time, even without active
intervention, the symptoms may disappear on their own, in
which case we would talk about spontaneous remission
of the illness. "Remission". Spontaneous
remission is surprisingly common in depression, which tends
to come and go in its natural course. But it also
takes time, maybe 6-9 months, so rather than wait the
illness out, it's probably better to get some sort of active
treatment.
Response. Now let's suppose that the patient
does receive some active treatment, whether it's
psychotherapy, or some kind of biological treatment, like
medication. Many patients will respond positively to
whatever treatment they receive. If they don't, the
therapist may switch to a different form of treatment -- a
different approach to therapy or perhaps a different drug --
until something seems to work.
Recovery. In depression, subjects may respond
positively after a couple of weeks of appropriate treatment,
but it may take a while before they really get back to
normal -- a complete recovery, in which they are symptom
free. Alternatively, may show a partial recovery, in
which some symptoms remit completely, but not others; or
there may be a clinically significant reduction in the
severity of symptoms. Sometimes, unfortunately,
recovery doesn't occur at all, in which case the patient
proceeds from an acute to a chronic illness, calling for
continuation treatment.
Relapse. Even with a complete recovery, there
is some chance that the symptoms may come back, perhaps not
as severely as before, but enough to interfere with normal
functioning. In depression, for example, the
likelihood of a relapse even after what appeared to be a
complete recovery is about nine times the risk of depression
occurring in the general population. Apparently the
acute episode is still going on, appearances to the contrary
notwithstanding. For this reason, most therapists
don't stop treatment immediately once the patient has
recovered, but continue it for a while.
Recurrence. Even after a patient has
completely recovered, there is still some chance that
another acute episode can occur later. If a person has
recovered from an acute episode of depression, there is
still a chance that another acute episode will occur --
about three times more risk than in the general
population. For this reason, even patients who have
completely recovered may want to maintain some degree of maintenance
treatment.
The first goal of treatment is to
achieve a cure. Genuine cures will do more than suppress
superficial symptoms: they will eliminate underlying
pathology, or reduce it to a clinically significant extent,
returning the person's level of functioning to "within normal
limits" even after active treatment has stopped. In the
absence of a cure, treatment focuses on the amelioration of
symptoms, or rehabilitation regimes that permit the patient to
cope with a chronic condition.
Custodial Care
Historically,
the scientific treatment of mental illness has come in three
basic forms.Up
until the 20th century, there were really no active
treatments available for mental illness, so intervention
focused largely on custodial care -- chiefly the warehousing
of the mentally ill in public hospitals or private asylums.Pennsylvania
Hospital, America’s first hospital, was founded by Benjamin
Franklin and Thomas Bond in 1751, when Pennsylvania was
still a British colony, for the care of the indigent and the
mentally ill.
Initially, the asylum was simply a separate ward in the
original hospital on Pine Street, later a separate wing,
the asylum was moved to the more rural West Philadelphia
in 1841, and in 1859 to its ultimate location (at 49th and
Market Streets).
Originally, the asylum housed
only dangerous and disruptive "lunatics", and the
primary "treatment" was restraint, along with purging
and bloodletting (the humor theory of disease was still
popular, and it applied to mental as well as medical
illnesses).
Benjamin Rush, a physician at the Pennsylvania
Hospital from 1783 to 1813 who was among the signers of
the Declaration of Independence, took such an interest
in the treatment of the mentally ill that he is now
considered the "father" of American psychiatry. In
many respects, Rush was a conventional physician for his
time, when the "standard of care" emphasized bleeding
and purging. On the other hand, he was the first
American physician to apply what we now call the
"medical" model, as opposed to the "moral" or
"supernatural" models, to mental illness. His view
that mental illnesses were true "diseases of the mind"
which should be freed from moral stigma, and be treated
with medicine rather than moralizing, marks a shift from
the moral model of mental illness to the medical
model. Influenced by the Quakers who established
an asylum in the nearby Friends Hospital, Rush pioneered
a set of reforms for the treatment of the mentally ill
-- just as he had earlier reformed Pennsylvania's penal
system at the Eastern State Penitentiary. For
example, he established "day rooms" where patients could
be visited by family and friends, and have access to
books, game, and the like. Rush's first son, John,
apparently suffered from depression. After
attempting suicide in New Orleans in 1810, he was
brought home to Philadelphia and lived at the
Pennsylvania Hospital until he died in 1837 (the elder
Rush himself died in 1813).
For recent biographies of
Rush, see Rush: Revolution,
Madness, and the Visionary Doctor Who Became a
Founding Father (2018) by Stephen Fried
and Dr. Benjamin Rush:
The Founding Father Who Healed a Wounded Nation
(2018) by Harlow Giles Unger.
Another set of reforms was
instituted by Thomas Story Kirkbride, who was the
founding superintendent of the new asylum in West
Philadelphia, then known as the Pennsylvania Hospital
for the Insane and later at The Institute of
Pennsylvania Hospital. Kirkbride had been a
medical resident at Friends Hospital, and was impressed
by the "moral treatment" of the patients there.
Like Pinel before him, Kirkbride freed even "dangerous"
patents from their restraints, and permitted to walk
around the wards outside their hospital rooms.
Patients on a ward took their meals together, instead of
in their separate rooms, and were encouraged to read,
play games, or work on the hospital grounds. In
1844, Kirkbride was one of the founders of the
Association of Medical Superintendents of American
Institutions for the Insane, which eventually became the
American Psychiatric Association. In 1854,
Kirkbride published his treatise On the
Construction, Organization, and General Arrangement of
Hospitals for the Insane, which set the standard
for state and private mental hospitals for many decades
-- so much so that the hospitals of this era are often
called "Kirkbrides". Kirkbride got to put his
ideas into practice when the new hospital was built in
1859. The hospital was deliberately placed far
from the center of town (which was true then), on a
piece of land so large as to contain gardens and even a
small farm, offering patients the opportunity to work
and play outside. There was a wall for security,
but it was placed so far from the hospital buildings as
to be unobtrusive. The buildings themselves were
completely up-to-date in terms of plumbing, heating,
ventilation, lighting, and the like. There were
two wings, one for each sex, with the most severely ill
patients placed on the ground floor farthest from the
central administrative offices, and the least impaired
on upper floors close to the core. The corridors
were wide, the ceilings high, there were lots of
windows, and lots of doors to the outside. There
was a library and a game room. Many of the staff
lived on the hospital grounds, including the
superintendent himself.
The Kirkbride model was
followed by at least 75 other private and public
mental hospitals in the latter portion of the 19th
century, including the Oregon State Hospital, which
was the setting for the film of Ken Keesey's novel, One
Flew Over the Cuckoo's Nest.
Another "Kirkbride", the
Buffalo State Asylum for the Insane (designed by the
great 19th century architect H.H. Richardson), is now
the Hotel Henry. St. Elizabeth's Hospital, in
Washington, D.C., is slated to become the new
headquarters of the Department of Homeland Security
(no wisecracks!). I worked at the Institute as
a graduate student in the early 1970s, and it seemed
as much a resort as a hospital.
New
York Hospital and the Virginia Asylum were also chartered
for the care of “Lunaticks” before the Revolutionary War,
but did not open their doors until after the War was over.Still, the
patients there were mostly “warehoused”, out of sight of the
rest of the community.After the Civil War, Silas Weir Mitchell gave a more
positive spin to “warehousing” by prescribing a “rest cure”
for “mental exhaustion – famously depicted in The Yellow Wallpaper,
an early feminist classic by Charlotte Perkins Gilman.
For insight into the state mental
hospital system, see The Lives They Left Behind:
Suitcases from a State Hospital Attic by Darby
Penney and Peter Stastny (2007), based on artifacts
collected from Willard State Hospital in Romulus, New
York. Link to the accompanying website: www.suitcaseexhibit.org.
Beginning in December 2013, this exhibition can be
viewed at the Exploratorium in San Francisco.
For a biography of Thomas Kirkbride, see the Art of
Asylum-Keeping: Thomas Story Kirkbride and the Origins
of American Psychiatry by Nancy Tomes.
Sometimes, the mentally ill were confined at home, in
back bedrooms and attics, as in the character of Mrs.
Rochester in Charlotte Bronte's Jane Eyre (1847)
-- the original "madwoman in the attic".
Beginning
in the late 19th century, various forms of psychotherapy
were introduced.These
interventions, one way or another, were intended to alter
the patients' pathological mental states -- their abnormal
beliefs and feelings and desires, which were thought to
underlie the various symptoms of mental illness.By changing these
abnormal, maladaptive mental states, mental health
professionals sought to change the maladaptive patterns of
behavior that brought patients to the attention to the
professionals in the first place.Beginning in the
20th century, a wide variety of biological treatments were
introduced for mental illness.These began with procedures like electroconvulsive
therapy, and even psycho-surgery where physicians operated
on various brain centers that were presumed to be implicated
in the patient's problems.But more recently, a wide variety of medications have
been introduced for the treatment of various metal
illnesses, beginning with schizophrenia.These medications
have largely supplanted psychosurgery and ECT, though both
still have a place in selected cases.
For histories of the beginnings of mental-health
treatment in America, see:
American Nervousness: Its Causes and Consequences
by George M. Beard (1881 -- note the date!);
American Nervousness, 1903 by Tom Lutz (1991).
Before Prozac (2008) and How Everyone
Became Depressed: the Rise and Fall of the Nervous
Breakdown (2013) by Edward Shorter, the
pre-eminent historian of the psychiatry in America.
Beginning in the mid-20th century,a wide variety of psychotropic
medications were introduced for the treatment
of various mental illnesses, beginning with schizophrenia.
Mental health has been a full participant in the
"pharmaceutical revolution" that has swept modern
medicine.
The use of biological treatments for mental illness flows from
the assumption that mental illnesses have biological causes --
that they are, in effect, diseases of the nervous
system. For an excellent history of the search for
biological causes of and treatments for mental illness, see The
Mind Fixers: Psychiatry's Troubled Search for the Biology of
Mental Illness by Patricia Harrington, a historian of
medicine at Harvard (reviewed by R.J. McNally, a clinical
psychologist, in the Wall Street Journal, 05/04/2019;
by Jerome Groopman, a physician, in the New Yorker,
05/27/2019; by Gary Greenberg, a psychotherapist and author of
The Book of Woe: The DSM and the Unmaking
of Psychiatry, in The Atlantic,
04/2019; and by Galvin Francis in the New York Review of
Books, 01/14/2021).
Harrington points out that the very first biological
theory of mental illness was for syphilis, a venereal
disease whose late stages were marked by dementia and
delusions, as well as motor problems -- the "general
paresis [paralysis] of the insane". By the late 19th
century, this diagnosis was applied to as many as 20% of
new patients entering insane asylums. Richard von
Krafft-Ebing (yes, that Krafft-Ebing) proved that
syphilis was the specific cause of general paresis -- the
first time that a specific biological cause had been
identified for any form of mental illness.
Identifying the pathogenesis -- the medical term for a
biological cause -- of general paresis stimulated similar
searches for the pathogenesis of other forms of mental
illness, but these were largely unsuccessful. The
reason, Harrington thinks, was that physicians focused
mostly on anatomy, looking for lesions and other
pathologies in brain tissue. Advances in medical
bacteriology eventually led some biologically oriented
psychiatrists to argue that mental illnesses were caused
by microbes arising from other parts of the body --
leading to experimental treatments involving the removal
of teeth, ovaries and testes, and parts of the digestive
system. None of these treatments were effective, of
course. Theories based on pathological anatomy were
revived when Egas Moniz received the 1949 Nobel Prize in
Physiology or Medicine by inventing the lobotomy, in which
the prefrontal cortex was effectively disconnected from
the rest of the brain (most notoriously by Walter Freeman,
an American neurosurgeon, using a tool resembling nothing
more than an ice pick inserted into the brain through the
patient's eye socket).
At the same time, more psychologically oriented
physicians, such as Jean-Martin Charcot, Pierre Janet, and
most famously Sigmund Freud, argued that some forms of
mental illness, such as hysteria (as it was called then),
could arise from psychological as well as biological
causes -- especially sexual trauma of various kinds.
Hysteria was labeled a "functional" disorder, The apparent
success of Freudian psychoanalysis caused many
psychiatrists to turn away from physiology toward
psychology. Psychoanalysis -- as both a theory of
and a treatment or mental illness -- dominated psychiatry
for most of the 20th century. After World War II, ,
during what W.H. Auden famously called "The Age of
Anxiety", neo-Freudian psychoanalysts focused focused on
real-life anxiety, and the need for emotional security,
rather than the repression of sexual fantasies and
experiences as the cause of neurosis -- while conceding
that psychosis probably had biological causes. Then
again, it was around this time that "schizophrenogenic"
mothers were blamed for causing schizophrenia in their
children by placing them in a "double bind" of conflicting
messages; and "refrigerator mothers" were blamed for their
children's autism.
Some psychiatrists tried to form a middle way between
biology and psychology. For example, Adolph Meyer
advocated a "psychobiological" approach that acknowledged
both physiology and biology, and a "common sense" approach
to mental illness that eschewed dogmatic positions in
either direction.
The 1960s saw a number of attacks on institutional
psychiatry:
Thomas Szasz, in The Myth of Mental Illness
(1961) argued that mental illness was just that -- a
myth;
Erving Goffman, in Asylums (1961), compared
mental hospitals to concentration camps and other "total
institutions" that deprives their inmates of any
personal autonomy;
Michel Foucault, in Madness and Civilization
(1961; this was a very big year for critiques of
psychiatry) portrayed the mentally ill as an oppressed
group and psychiatrists as their oppressors;
feminists such as Betty Friedan (in The Feminine
Mystique, 1963) criticized psychiatry for putting
the blame for mental illness on mothers.
In the 1970s, the Insane Liberation Front and other
activists argued that "mental illness" was a label
applied to nonconformists in order to deprive them of
their freedom.
The crisis of psychiatry came to a head in 1972, when
the American Psychiatric Association voted to remove
homosexuality from its official list of mental
illnesses. Ironically, the decision was the correct
one: homosexuality is no more "pathological" than
heterosexuality. But science doesn't put things to a
vote: it has objective standards for discerning truth from
falsehood. The fact that this issue had to be put to
a vote revealed that there were no objective
standards for what constituted a mental illness, and
undermined claims that psychiatry was a science-based
discipline.
The dominance of psychoanalytic psychiatry was broken by
two events -- first, the development of new drugs for the
treatment of anxiety (e.g., Valium), depression (e.g.,
Elavil), and schizophrenia (e.g., Thorazine); and second,
by the invention of behavior therapy (and later cognitive
behavioral therapy). The first stimulated a new
generation of biological theories of mental illness -- if
mental illness could be treated with a pill, then its
pathogenesis must lie in physiology, if not anatomy.
The second provided an alternative to psychoanalysis --
and one that was more effective than psychoanalysis, to
boot.
Psychiatry's scientific status was restored, to some
extent, with the publication in 1973 of the 3rd edition of
the Diagnostic and Statistical Manual of Mental
Disorders, which eliminated all reliance on
psychoanalytic theory and focused on a purely descriptive
classification of various forms of mental illness in terms
of their characteristic symptoms such as anxiety,
depression, or delusions.
The apparent success of anti-anxiety,
anti-depressant, and antipsychotic medications stimulated
a new round of biological theories of mental
illness. The logic went like this: Elavil increases
levels of norepinephrine, and helps alleviate depression;
therefore, depression must be caused by diminished levels
of norepinephrine. It's bad logic, of course.
And despite years of searching, there's no good evidence
that norepinephrine levels are related to
depression. A similar argument, similarly flawed
both logically and empirically, was employed with
selective serotonin reuptake inhibitors (SSRIs) were
introduced for depression. Despite widespread
adoption of medication as a treatment of for mental
illness, there is still no definitive evidence that
chemical imbalances cause mental illness. They
remain "empirical" treatments -- they work, apparently,
but there's no theory that explains why they
work.
And even when it comes to purely empirical treatments,
the pharmaceutical industry appears to be at a dead
end. The latest fads in biological psychiatry
involve genes, gut bacteria, and the immune system.
Still, Harrington quotes Steven Hyman, once the director
of the National Institute of Mental Health, that "no new
drug targets or therapeutic mechanisms of real
significance have been developed for more than four
decades".
Empirical treatments aren't bad: medicine offers lots of
them, and they really work. But understanding the
nature of mental illness -- well, that's still a
puzzle. It's a puzzle that psychology tries to help
solve. At the end of her book, Harrington expresses
the hope that psychiatry will "overcome its persistent
reductionist habits and commit to an ongoing dialogue
with... the social sciences and even the
humanities". That's where psychology -- which,
remember, is both a biological science and a social
science, all wrapped up in a single package -- can help.
Biological Treatments
Where biological causes are the primary
factor in mental illness, strictly biological treatments may
effect a complete cure. Of course, such biological cures
require an understanding of the biological basis of some form
of mental illness.
Biological cures are
exemplified by treatments available for two specific forms of
intellectual disability.
Phenylketonuria is a metabolic disorder that
interferes with the myelinization of neural tissue. If a
child with phenylketonuria is put on a strict low-protein
diet until about age 6, this form of intellectual
disability can be prevented entirely. Unfortunately
individuals with PKU must stay on a somewhat restricted
diet for the rest of their lives. In 2007, the Food and
Drug Administration approved Kuvan, the first drug
treatment for the disorder, while will allow for a
somewhat more relaxed dietary regimen, allowing affected
individuals to eat things like cheese and pizza (if only
in moderation).
Cretinism, another form of intellectual
disability, is caused by thyroxine deficiency, a hormone
imbalance due to a lack of iodine in a pregnant woman's
diet. This illness can be prevented entirely by treating
the infant with thyroid extract during the first year of
life (it can also be prevented entirely by giving the
mother the iodine she needs during pregnancy).
There are many other biological
treatments for mental illness, including many different
medications but also psychosurgery and electroconvulsive
therapy. These are often very effective, but they do not reach
the level of a cure, because the illness returns when the
treatment is discontinued.
Psychosurgery, especially prefrontal
lobotomy (the destruction of the prefrontal cortex of
the brain) was once rather popular: Egas Moniz, the Portuguese
neurologist who pioneered the technique of "prefrontal
leukotomy", even won the Nobel Prize for Physiology or
Medicine in 1949. The technique has now been completely
repudiated, and Moniz' prize considered something of an
embarrassment. However, as our understanding of brain
function advances more nuanced surgical approaches to mental
illness are sometimes proposed. For a history of
psychosurgery, see Great and Desperate Cures: The Rise and
Decline of Psychosurgery and Other Radical Treatments for
Mental Illness (1986) by Elliot Valenstein, a
distinguished neuroscientist. Valenstein's other books are
also of interest:Brain Control: A Critical Examination of
Brain Stimulation and Psychosurgery (1977) and Blaming
the Brain : The Truth About Drugs and Mental Health
(1998).
Although nobody does lobotomies anymore,
psychosurgeries are still performed (of course, brain surgery
is frequently performed for strictly neurological disorders
like epilepsy). Most of these operations occur in cases
of obsessive-compulsive disorder or depression, and they are
pretty rare -- although, with increasing evidence of efficacy
and safety, their use is increasing (though they are not
risk-free). Most of these "surgeries" are performed by
means of electrical stimulation through microelectrodes, as
opposed to with a scalpel (as was the case, for example, with
the earlier lobotomies).
Cingulotomy, destruction of a portion of
the anterior cingulate gyrus, which disrupts a
circuit that connects emotional enters in the limbic
system to the frontal cortex.
A related procedure, known as capsulotomy,
targets the internal capsule, a bundle of white
matter that connects midbrain and forebrain structures.
One new form of surgery involves deep brain
stimulation -- surgically implanting electrodes in
the brain, using much lower levels of current to stimulate
specific brain areas -- sort of like the pacemakers that
are implanted to treat certain forms of heart
disease. Originally developed as a treatment for
Parkinson's disease, and later extended to Tourette's
syndrome (both more properly regarded as neurological
syndromes with behavioral consequences than as mental
illnesses per se), deep brain stimulation is now
being performed in some cases of depression and
obsessive-compulsive disorder as well.
For depression, the electrodes are typically implanted
in the subcallosal cingulate gyrus (Brodmann's area 25).
For a a recent discussion of this technique, which
as of 2015 had not yet been approved for routine
therapeutic use, see "Treating Depression at the
Source" by Andres M. Lozano & Helen S. Mayberg, Scientific
American, 02/2015.
A variant on deep-brain stimulation for depression,
which has been approved for routine use, is transcranial
magnetic stimulation, stimulates the brain with
short bursts of magnetic pulses focused on the left
prefrontal cortex -- a little like electroconvulsive
therapy, though without the convulsive seizures or
transient confusion and memory loss.
Both DBS and TMS have been proposed for use with
depressed patients who are not responsive to
conventional psychotherapeutic or pharmacological
treatments.
For obsessive-compulsive disorder, the electrodes are
implanted in the nucleus accumbens.
A newer technique, which doesn't employ electrical
stimulation at all, is gamma knife surgery,
derived from a radiological treatment for cancer, which
focuses a large number of beams of radiation on a very
small area of brain tissue. Each beam is, itself,
completely benign, but the cumulative effect of all the
beams is sufficient to destroy tissue precisely at the
point of focus.
The treatments are strictly
experimental, and they can have powerful and unpleasant
side-effects, so they are typically performed only under a
"humanitarian device exemption", where no other treatment has
worked. For this reason, deep brain stimulation has not
been subject to the kinds of controlled clinical trials that
are required for approval of new medications and other medical
treatments.
Electroconvulsive Therapy (ECT)
is sometimes used as a treatment for severe depression. ECT
employs a brief electrical current applied to the scalp to
induce a brief seizure somewhat similar to that seen in
epilepsy. ECT has a somewhat unsavory history, having been
misused in the past, but the fact is that a short course of
ECT, judiciously applied, can often produce rapid remission of
depressive symptoms. ECT is often avoided because of its
presumed side-effects, which (when misapplied) can include
brain damage. However, ECT does not hurt (because the patient
is unconscious during the treatment). ECT applied bilaterally
(with electrodes placed on both sides of the head) can produce
an amnesia similar to that which occurs following a concussive
blow to the head; but memory impairment can be reduced
substantially if the treatment is applied unilaterally, so the
seizure is confined to one (usually the non-dominant)
hemisphere. Biologically, ECT increases levels of
norepinephrine and serotonin in the brain, which is
interesting in light of the "monoamine" hypothesis of
depression.
ECT and TMS are sometimes referred to as "jump-starting
the brain", but we don't really have a good idea why they
work -- when they do.
By far the most popular and effective
biological treatments for mental illness involve psychotropic
or psychoactive medications: beginning in
the 1950s, psychiatry has been a full participant in the
"pharmaceutical revolution" in medicine.
A
variety of antipsychotic medications are used in the
treatment of schizophrenia. Most common, perhaps, are
the phenothiazines, which appear to decrease dopamine
levels in the brain. Typical brand names are Thorazine,
Stelazine, Prolixin, and Mellaril. Haldol (a butyrophenone),
and Navane (a thioxanthene) are also widely used. There is
also a group of "atypical" antipsychotics like Clozaril,
Resperidal, Zyprexa, and Abilify, which are as effective as
the earlier antipsychotic agents, but cause fewer
side-effects.
To be honest, though, most of the drugs
used in the treatment of schizophrenia are really nothing more
than major tranquilizers, which calm the patient, reducing the
tendency to report and act on hallucinations if not to have
them.Setting aside the dopamine hypothesis of schizophrenia,
nobody thinks that these drugs act directly on the patient's
underlying pathology. However, these drugs do make patients
more manageable, and their introduction made everybody's life
better, staff and patients, inside mental hospitals -- and
made it possible for many people with schizophrenia to be
released from mental hospitals to live with their families or
elsewhere in the community. But, as with many psychiatric
drugs, you've got to keep taking them. And once released from
direct supervision, this is something that many schizophrenics
just aren't inclined to do.
A
major revolution in the treatment of depression came
with the introduction of antidepressant drugs.
The tricyclic antidepressants, drugs like
Elavil, Tofranil, and Sinequan, increase levels of
norepinephrine and serotonin.
Another group of antidepressants, known as the MAO
inhibitors -- Nardil and Parnate are examples
-- inhibit monoamine oxidase, a substance which, in turn,
deactivates norepinephrine and serotonin. Both the
tricyclics and the MAO inhibitors act by increasing the
release of norepinephrine and serotonin into the synapse
Recently, these earlier generations of drugs have begun
to be replaced by a newer generation of selective
serotonin reuptake inhibitors(SSRIs) such as
Prozac, Zoloft, Paxil, Celexa, and Lexapro. As their name
implies, these drugs act selectively on serotonin, and
have little or no effect on norepinephrine; and rather
than increasing the release of serotonin, they act to
prevent its reuptake by the presynaptic neuron -- thus,
effectively, increasing the levels of serotonin available
at the synapse.
There is also a class of drugs called selective
serotonin and norepinephrine reuptake inhibitors, or
SNRIs, such as Cymbalta, which act on both
serotonin and norepinephrine -- thus accomplishing the
same effect as the MAO inhibitors, but through a different
mechanism.
And, of course, there are now selective norepinephrine
reuptake inhibitors, also known as an NRIs,
including Strattera
The SSRIs and SNRIs are as effective as
the earlier tricyclics and MAO inhibitors -- a fact that has
led to the revision of the general monoamine hypothesis of
depression by the more specific serotonin hypothesis of
depression.
For a discussion of recent advances in the
drug treatment of depression, see
Lifting the Black Cloud" by R.M. Henig,Scientific
American, 03/2012.
Also within the category of mood
disorders,lithium carbonate has proved to be a very
effective treatment for bipolar disorder, also known
as "manic-depressive illness". Treatment with lithium reduces
or eliminates episodes of mania in as many as 70% of cases,
and also reduces episodes of depression. However, because
lithium is toxic, its use must be carefully monitored. Lithium
is another one of those psychiatric drugs which seem to work
-- in fact, it works very well, and works only for bipolar
disorder -- but we have no idea why it works, or what
bearing its effectiveness might have on our understanding of
the nature of mania or bipolar disorder. Certainly,
mania isn't caused by a lack of lithium in the body.
Just like Coca-Cola once actually
contained cocaine, so7-Up, another popular soft
drink once contained lithium. This just one of the fun
facts included in Lithium: A Doctor, a Drug, and a
Breakthrough (2019) by Walter Brown, a
psychiatrist. Discovered in 1949 John Cade, an
Australian psychiatrist, lithium was the very first
psychiatric drug to approach anything like a cure, as
opposed to mere symptom relief (remember, before this time,
all psychiatric medications were just tranquilizers).
And the research which first demonstrated its curative
effects, carried out by Mogens Schou, a Danish psychiatrist,
in 1954, were the first randomized, controlled clinical
trials of any psychiatric drug.
Similarly,
early drug treatment of anxiety disorder focused on
sedatives such as the barbiturates (e.g. Nembutol and
Seconol), propanediols (e.g., Miltown, Equanil), and
benzodiazepines (e.g., Librium, Valium, and Xanax). The
20th century was known as the "Age of Anxiety", and popular
literature and movies concerned with American middle-class in
the 1950s and 1960s are full of references to these drugs.
These drugs are also, essentially, tranquilizers -- though far
less potent than those used in the management of
schizophrenia. Specifically, they increase the activity of the
neurotransmitter GABA, which in turn suppresses activity in
the hypothalamic-pituitary-adrenal axis (HPA).
As with the antipsychotic medications,
there is also a group of atypical anxiolytics, such as
Buspirone, which are as generally effective as the earlier
sedatives but with fewer side-effects.
Whether "typical" or "atypical", all
psychotropic drugs in a particular class have the same basic
pharmacological mechanism of action:
The antipsychotics, like Thorazine, decrease levels of
dopamine.
The antidepressants, like increase serotonin, dopamine,
or norepinephrine.
The anxiolytics increase GABA.
Newer drugs within a class are
sometimes called "me-too" drugs, because they
all have the same basic effects -- put another way, the newer
drugs are little more than copycats of the older ones.
The newer drugs may have fewer side-effects, and be somewhat
safer and easier to tolerate. But the basic underlying
pharmacological action is no different. So why are new
drugs introduced? Mostly because the patents are running
out on the old ones. And, in fact, the pharmaceutical
industry isn't devoting that much research to the development
of truly new psychotropic drugs, because -- despite their
popularity -- there isn't that much to be gained financially
from them. There is much ore money to be made from drugs
that treat cancer, heart disease, or diabetes.
Because of the co-morbidity between
anxiety and depression, anxiety disorder is sometimes treated
with SSRIs such as Paxil. The rationale for this strategy
isn't completely clear -- maybe it's to help patients feel
less depressed about being anxious!
In many instances, specific drug
treatments are developed based on a specific somatogenic
theory of the illness in question. In theory, at least,
psychotropic medications work because they address the
biological bases of mental illness. Thus, according to the
dopamine hypothesis of schizophrenia, drugs that alter the
processing of dopamine should be effective treatments for
schizophrenia but not depression; and according to the amine
hypothesis of depression, drugs that alter the
processing of monoamine neurotransmitters should be effective
treatments for depression but not for schizophrenia. The
SSRIs, which act specifically to enhance the availability of
serotonin in depressed patients, are perhaps the clearest
expression of this connection between theory and treatment.
But sometimes drug treatments are simply empirical,
meaning that they are prescribed simply because they are known
to help, and not because their efficacy is predicted by any
theory of the illness in question.
A good example of such an empirical
treatment is the prescription of amphetamine, such as Ritalin,
for the treatment of ADHD.
A report by Bradley (1937) had noted that Benzedrine, a
trade name for amphetamine, had positive, and paradoxical,
effects on a group of schoolchildren with various
"behavioral issues" -- what we would now recognize as
ADHD. Bradley originally prescribed the drug to treat
headaches, and noticed that it affected their behavior as
well.
That same year, interestingly, news media carried
reports of college students taking amphetamine as a study
aid. Plus ca change....
Ritalin, another proprietary form of amphetamine, was put
on the market in 1956, and a study soon showed that it, too,
produced positive effects on children with various
behavioral disturbances (Ritalin was named after the wife of
the chemist who formulated the drug).
In 1970, amphetamines were placed under tight restrictions
(Schedule II) by the Controlled Substances Act.
Initially, sales of Ritalin and other amphetamines declined
substantially, but recovered as more children were diagnosed
with hyperactivity disorder or ADD/ADHD.
Another proprietary amphetamine, Adderall, was introduced
in 1996. Essentially the same drug was formerly
marketed as Obetrol, for the control of obesity; its new
name is a contraction of "ADD for all", which should tell
you something.
Concerta was introduced in 2000.
The landmark "MTA" study (the acronym stands for
"Multimodal Treatment of Children with ADHD") found that 68%
of children who received Ritalin or Concerta with behavior
therapy showed improvement; comparable figures for
medication alone were 56%, behavior therapy alone 34%, and
25% for an untreated control group. This study
effectively set medication as the "standard of care" for
ADHD.
There's no good reason why Ritalin
should work in these cases -- and given that amphetamine is a
central nervous system stimulant, there would be every good
reason to think that it would make things worse. Such
"off-label" use of medications is a fairly common practice in
medicine: physicians may "experimentally" prescribe drugs for
conditions other than those indications approved by the Food
and Drug Administration following controlled studies of safety
and efficacy). But exactly how it occurred to anyone to try
Ritalin in the first place isn't clear. Perhaps it was simply
an act of desperation after everything else failed. But it
does work, at least for many patients with ADHD, and is now
the standard of care for both children and adults carrying the
diagnosis -- ADHD is now a "labeled" indicator for Ritalin and
similar drugs, rather than an "off-label" use. But there's
still no theory that explains the paradoxical effects of
Ritalin on ADHS. One theory is that amphetamines activate
brain centers for the control of attention which are
relatively inactive in patients with ADHD -- but this is just
a theory, and a rather post-hoc one at that, and as yet
there's no evidence supporting it.
Actually, there is a double
paradox here, because the evidence for the efficacy of
amphetamines in the treatment of ADHD is somewhat
ambiguous. Laboratory tests show that Ritalin (and
similar drugs) improves performance on laboratory tests of
attention and working, and also has positive effects on brain
centers involved in these cognitive functions. But other
studies show that there is no corresponding improvement in
student academic performance, as measured by grade-point
averages, achievement-test scores, or even the likelihood of
repeating a grade. of elementary and secondary-school.
So, whatever is going on in the laboratory, and the brain,
doesn't seem to translate into the real life of the
classroom. One possibility is that these children, and
their families, come to rely too heavily on the drugs.
In the absence of proper study skills, and a home environment
conducive to and encouraging of study, academic performance
won't improve just by taking a pill.
Notes on Cosmetic Neurology
Advances in neuroscience, pharmacology, and gaming have
conspired to usher in a new age of what can only be called
cosmetic neurology (Chatterjee, 2004, 2007) -- that
is, the use of neuroscientific and pharmaceutical
techniques to enhance performance in healthy people --
much like cosmetic surgery is intended to enhance physical
appearance in healthy clients who have "normal" physical
traits. Cosmetic neurology raises a host of ethical
issues, but the first issues they raise are scientific and
medical -- namely:
Do these techniques work?
Do they do any harm?
What are the cost-benefits ratios attached to them?
Let's look at some cases.
1. "Study Drugs"
Actually, a number of "stimulant" drugs are
now prescribed for ADHD, including methylphenidates
such as Ritalin, Focalin, and Concerta, and amphetamines
such as Adderall and Vivanse. All have the "paradoxical"
effect of focusing the concentration of patients with ADHD.
But maybe these "paradoxical" effects are not paradoxical at
all, and that these and other drugs may
improve focus and concentration in anyone.
Other psychostimulants include:
Modafinil (trade name Provigil),
used in the treatment of narcolepsy and excessive
sleepiness.
Donepezil (trade name Aricept),
used in the treatment of Alzheimer's disease.
In fact, these alleged "brain boosters"have
been increasingly used by high-school and college students
who do not have ADHD as "study drugs" -- that is, as
pharmaceutical aids for studying and test-taking. Students
have been known to fake the symptoms of ADHD in order to get
a prescription, and there is apparently a vigorous black
market in the drugs. A 2007 survey by the Centers for
Disease Control and Prevention found that 2.7 million
children and adolescents were taking prescribed medication
for ADHD. Some of that medication, perhaps as much as
20%, is "diverted" to others for non-prescribed use.
In addition, some students persuade their family physicians
to prescribe stimulants to help them get through academic
exercises such as the SAT.
It should be noted, first of all, that these
drugs are controlled substances (in Schedule II, right up
there with cocaine and morphine): possession and use without
a prescription is illegal, and even giving them away can
lead to felony charges.
It should also be understood that, like all
psychoactive drugs, there is a danger of addiction.
Habitual overuse of stimulants can lead to episodes of
psychosis, and even suicide. So stimulants should
never be taken unless actually prescribed by a physician;
and the medication regime should be continually
monitored. N For a cautionary tale, see "Drowned in a
Stream of Prescriptions" by Alan Schwartz (New York Times,
02/03/2013) -- the cautionary tale of Richard Fee, the
pre-med president of his college class, who faked ADHD to
get a prescription for Adderall, and hanged himself when his
prescription ran out.
These are powerful
drugs. And this is your brain, and you only get one
of it.
From a scientific point of view, it has to
be said that, until recently, claims about the effectiveness
of Ritalin and similar drugs as study drugs for "normals"
are largely anecdotal. A formal review of this literature by
Elizabeth Smith and Martha Farah (Psychological Bulletin,
2011). They found that there was little
evidence that stimulants improved the cognitive performance
of normal, healthy individuals. There may be some
positive effects, but they seem to be small and variable,
and do not necessarily translate into improved academic
performance.
From a medical standpoint, however, it
should be understood that, like all psychoactive drugs,
these substances have negative side effects. Chief among
these are that they are highly addictive. It is very easy
for students to become dependent on these drugs, and for
their prolonged use to lead to the addictive cycle of
tolerance and withdrawal.
So, the word from here is: as tempting as it
may sometimes be,don't do it; don't even start.
Just study hard and do your best!
For a discussion of the scientific and ethical
issues involved, see:
"Turbocharging the Brain" by Gary Stix,Scientific
American, October 2009.
ADHD Nation: Children, Doctors, Big Pharma, and the
Making of an American Epidemic (2017) by Alan
Schwarz, based on a series he wrote for the New York
Times in 2012. Schwarz is clear that ADHD is
a legitimate diagnosis, and he acknowledges that
methamphetamines can be an effective treatment for the
disorder. But he also thinks that the syndrome is
vastly over-diagnosed, and that Ritalin and similar
drugs are vastly over-prescribed, leading to a serious
epidemic of drug abuse.
2. "Brain Training"
"Smart drugs" may not be the only way to
enhance cognitive performance (if, in fact, that's what they
do). Lately, some entrepreneurial psychologists have
begun to promote "brain training" programs, ostensibly based
on cognitive neuroscience. These are, essentially,
adult video games, aimed especially at baby-boomers (like
yours truly), and intended to stave off the cognitive
decline that comes naturally with age -- not to mention
Alzheimer's disease. Also to promote things like
"neuroplasticity", "fluid intelligence", and "working
memory"
These products go by a number of brands.,
most of which is some variant on "Brain Fitness".
According to a report by Sharp Brains, an industry group,
more than $1 billion was spent on brain-fitness programs of
various sorts, mostly software, in 2012 alone -- and the
industry is expected to reach $6 billion by 2020. I
don't intend to promote or criticize any particular product,
but I do want to offer some cautions about the whole
enterprise of "brain training".
One leading product is BrainHQ, sold by Posit Science,
co-founded by Michael Merzenich, a neuroscientist at UC
San Francisco.
Another is Lumosity, offered as a subscription service,
with new "brain games" every month.
There are lots of others, some with UC or Stanford
connections.
The rationale for these programs is simple
enough. We know from the literature on brain
plasticity that mental exercise can stimulate the growth of
neural connections, if not neurogenesis itself. And
these exercises do activate brain regions, especially in the
prefrontal cortex, that are known to be involved in working
memory, attention, and other executive functions.
Therefore, it only makes sense that these games would result
in improvements in brain function.
But, at least as of 2013, none of the
commercially available programs has received anything like
the kind of approval that new drugs must receive from the
Food and Drug Administration. Most of the research
demonstrating their effectiveness is proprietary, and has
not been subjected to peer review. And while the
published studies may report statistically significant
increases in brain activity, or gains in performance on
cognitive tasks, they don't necessarily show that these statistically
significant improvements lead to clinically
significant improvements outside the laboratory, in the
ordinary course of everyday living. Nor, for the most
part, have the published studies shown that using the
(fairly expensive) games produces improvements in
performance over and above any other kind of mental
exercise, such as doing a crossword puzzle, watching Jeopardy!
and Wheel of Fortune -- or, for that matter,
engaging in physical exercise for 30 minutes a day, five
days a week.
The rationale for "brain games" appears to be
be based on the idea that the brain is a muscle, which is
strengthened by use and weakened by disuse (a principle
you'll remember from Thorndike's Law of Exercise, translated
into neuroscientific terms). And it's rue that
practice on a task will make you better at that task -- and
with enough practice (like the "10 Thousand Hour Rule"),
even automatize the underlying processes such that task
performance occurs automatically, and consumes few or no
cognitive resources -- thus freeing up those resources to be
devoted to some other task. But the analogy is
inexact. We know from the Doctrine of Modularity that the
brain isn't like a muscle: if anything, it's like a whole
collection of muscles, each corresponding to a module.
The human body contains about 650 different skeletal
muscles, after all (maybe more, depending on how you count,
and we're not counting involuntary muscles, such as the ones
in the heart). There's no reason to think that
exercising the triceps brachii of the upper arm has any
effect on the triceps surae of the leg. You've got to
exercise them both, if you want to increase your total body
strength.
Another, related point: practice with any
game will make you get better at that game. That's
just learning. But there is little evidence that
getting better at any game actually improves cognitive
abilities or overall brain function.
So, as with any other treatment, drug, or
psychotherapy, or brain-fitness software, caveat emptor
-- which, freely translated from the Latin, means check
out the efficacy studies.
And, in fact, as of early 2017, there was
precious little evidence that these "brain-training"
programs actually accomplish their goals. Playing a
particular game may enhance a person's ability to perform
the tasks required by that particular game (no surprise
there!), but there is little evidence that the skills
acquired in one game generalize to other cognitive skills --
let alone prevent Alzheimer's Disease.
In October 2014, a large group of cognitive
psychologists and cognitive neuroscientists, organized by
the Stanford Center for Longevity and the Max Planck
Institute for Human Development issued "A
Consensus on the Brain-Training Industry from the
Scientific Community" arguing that claims that
"brain games" can "reduce or reverse cognitive decline"
are unsupported by scientific evidence from controlled
experiments. In response, another 100 cognitive
psychologists and cognitive neuroscientists published an open letter
attempting to make the case that cognitive training
actually improves cognitive function.
In December of that same year, however, a large
international group countered that "a substantial and
growing body of evidence shows that certain
cognitive-training regimens can significantly improve
cognitive function, including in ways that generalize to
everyday life".
On January
5, 2016, the Federal trade Commission fined the creators
and marketers of Lumosity, a popular
"brain-training" program, $2 million for deceptive
advertising (actually, the initial fine was for $50
million, but after the FTC discovered that Lumosity had no
hope of ever paying it, the fine was reduced to something
more manageable). The FTC determined that Lumos
Labs, the makers of Lumosity, had systematically deceived
its 1,000,000+ subscribers, who paid $14.95/month -- you
do the math -- by making "unfounded claims that Lumosity
games can help users perform better at work and in school,
and reduce or delay cognitive impairment associated with
age and other serious health conditions".
A comprehensive review by Daniel Simons and his
colleagues concluded that there was "extensive evidence
that brain-training interventions improve performance on
the trained tasks, less evidence that such interventions
improve performance on closely related tasks, and little
evidence that training enhances performance on distantly
related tasks or that training improves everyday cognitive
performance." They also found "that many of the
published intervention studies had major shortcomings in
design or analysis that preclude definitive conclusions
about the efficacy of training, and that none of the cited
studies conformed to... the best practices... essential to
drawing clear conclusions about the benefits of brain
training for everyday activities" ("Do 'Brain-Training'
Programs Work?", Psychological Science in the Public
Interest, 2016).
So what are the problems with
brain-training? Chiefly, purveyors of brain-training
games, like Lumosity, have not conducted proper research,
modeled after clinical trials, to demonstrate that their
products actually are effective.
True, customers who practiced their games, like one in
which they were asked to remember the location of colored
squares on a grid, got better at those games, and other
games very much like them (what is known as "near
transfer"); and they might have felt,
subjectively, that their cognitive skills had
improved.
But there is no evidence that these gains generalize
beyond the games themselves ("far transfer") -- much less
that they stave off dementia or even normal age-related
cognitive decline.
Moreover, most of the available studies have employed
inadequate control groups, such as "no treatment"
controls, who do nothing while the experimental group is
playing the games. The best study would have a
placebo control, like a drug trial.
Cognitive training has potential, so it would
be too bad if actions like the FTC's stopped research and
development dead in its tracks. But at the same time,
the claims of the brain-training industry far exceed the
available evidence. Worse, it seems like the purveyors
of brain-training games haven't even tried very hard to
document the effects of their products. They have,
however, been very eager to take consumers' money.
For an interesting first-hand account of
some of these programs, see "Mentally Fit: Workouts at the
Brain Gym" by Patricia Marx, New Yorker,
07/29/2013.
See also "Can You Train Your Brain" by
Simon Makin, Scientific American, July/August
2015.
3. TDCS
Another fad has been Transcranial
Direct Current Stimulation (TDCS), in which a low
electrical current is applied to certain brain areas --
e.g., the left prefrontal cortex -- by means of electrodes
attached to a power source (often, nothing more than a
9-volt battery!) and an interface which controls the amount
of current and the duration of stimulation. Sort of
like EEG in reverse, but not nearly as strong as
Transcranial Magnetic Stimulation. You can buy these
things on the market (e.g., the Foc.us), or make them at
home, and a recent review shows that it might actually
improve performance on some cognitive tasks (Chrysikou et
al., 2013). But as of 2013 the device was not approved
by the Food and Drug Administration, and because the device
is so new there is no data on any harmful effects of
long-term use -- and there is every reason to think that the
long-term effects can be very harmful indeed.
4. "Baby Apps"
While we're on the subject, there has been a
proliferation of baby apps for smartphones and
tablets, advertised as enhancing infants and children's
cognitive skills. The progenitors of these were the 'Baby
Einstein" videos marketed in the days before smartphones and
tablets. These days, "baby apps" are promoted as ways
to teach infants motor and spatial skills, numbers, and
language.
Again, on first blush, the idea seems
plausible. But in fact, there is very little evidence
that these "baby apps" do what is claimed for them.
The published research is paltry and ambiguous, and even
some of the software developers admit that they don't have
the research to back up their claims. These apps may
entertain and distract children, but there is no good
evidence that they actually teach them anything.
Mostly, it seems, they make parents feel better about using
screens to distract their kids during dinner or cocktail
hour.
And there are some reasons to think that they
may actually be harmful, by consuming time and effort that
might actually be devoted productively to creative play,
person-to-person interactions with parents and older
siblings, and the like. The American Academy of
Pediatrics recommends that children not be exposed to
"screen media" of any kind, including television, for at
least the first 30 months (2-1/2 years).
In 2013, the Campaign for a Commercial-Free
Childhood, an advocacy organization, filed a complaint with
the Federal Trade Commission intended to put the brakes on
the "baby genius industry". Either they provide
evidence to back up their claims, or they stop making the
claims. The group was successful in an earlier effort
against the "Baby Einstein" videos, forcing the Walt Disney
Company to offer refunds to consumers who bought them for
their educational value.
So, to repeat: As with any other treatment,
drug, or psychotherapy, brain-fitness or educational
software, or indeed any innovation of this sort, caveat
emptor -- which, freely translated from the Latin,
means What's the evidence?
The
pharmaceutical revolution in mental health has been a genuine
revolution, providing a degree of symptom relief that simply
was not available previously, and enabling the
de-institutionalization of large numbers of patients from
mental hospitals, which offered mostly custodial care, back to
their homes and into the community; it also improved the lives
of a large number of individuals who were being treated on an
outpatient basis by psychiatrists and other mental health
professionals.
The effectiveness of these
drugs also has theoretical implications for our understanding
of the biological mechanisms involved in certain forms of
mental illness.
The effectiveness of the phenothiazines supports the
dopamine hypothesis of schizophrenia.
The effectiveness of the tricyclics supports the
monoamine hypothesis of depression, just as the
effectiveness of the SSRI supports the revised serotonin
hypothesis.
The effectiveness of the benzodiazepines supports the
GABA hypothesis of anxiety.
In theory, these drugs attack the
biological bases of the symptoms of these disorders -- the
biological bases of their underlying psychological deficits.
But note that the reasoning here is somewhat circular: How do
we know that dopamine is implicated in schizophrenia? Because
the phenothiazines, which act on dopamine circuits in the
brain, are effective in the treatment of schizophrenia. Why do
the phenothiazines work so well? Because excess dopamine is
the cause of schizophrenia. What we really need is independent
evidence that these neurotransmitters are specifically
involved in these forms of mental illness.
Getting Past the Blood-Brain Barrier
Psychotropic
drugs are typically delivered through pills or
injection, but either way they have to get to the
brain to be effective. Technically, that's a
problem because the brain has a built-in defense
against foreign substances, known as the blood-brain
barrier (BBB). The blood vessels in the
brain are structured somewhat differently than those
found elsewhere in the body. They are lined with
a tightly packed sheath of lipid (endothelial) cells
that prevent pretty much anything except oxygen and
glucose from getting through to the neurons.
Various pathogens and ions, as well as some proteins
that can harm neural cells, are filtered out.
And so are many potentially useful psychotropic drugs
-- which is one reason why psychotropic drugs are so
hard to develop. For a thorough discussion of
this problem, see "A
Barrier to Progress: Getting Drugs to the Brain" by
Rachel Brazil, Pharmaceutical Journal,
05/15/2017, from which the image is taken.
Fortunately, there are ways around -- or, more
accurately, through the BBB.
Some molecules pass through because they're
soluble in water: they can cross the BBB on their
own, through a process known as paracellular
transport. This is very rare, because
the junctions between epithelial cells is very
tight.
Others are small enough that they are soluble in
lipids. Since the BBB is made up of lipid
cells, they pass through the epithelial cells
themselves -- diffusion. These drugs
include some antidepressants and many other
psychotropic drugs, including many addictive drugs
such as alcohol, nicotine, morphine, and heroin.
Other substances, such as biologics, which involve
lager molecules, can be carried through the
epithelial cells through specialized protein
transporters, such as amino acid chains, in
what is sometimes known as the "Trojan Horse
approach". There are a number of variants on
this "hitchhiker" strategy, but the
pharmacochemistry involved is much more than is
required at the level of an introductory psychology
course. This approach is especially popular
for delivering chemotherapy in the treatment of
brain cancer.
Finally, there are drugs that disrupt the
BBB itself, briefly opening a window that allows the
molecule through the epithelial cell.
This
last technique offers clues to the pathology of
Alzheimer's disease (AD) and other dementing
illnesses. The whole point of the BBB is to
prevent toxins and other harmful substances from
reaching the brain. If you disrupt the BBB, then
you open up the opportunity for such substances to get
in. There is already evidence that the BBB
deteriorates with age. This can allow proteins
such as albumin, which ordinarily cannot cross the
BBB, to get through, initiating a sequence of events
that can result in the brain damage seen in dementia
-- like the plaques that are characteristic of
AD. So, one approach to treating, or perhaps
preventing, AD is to find a way to "plug" the leaks in
the BBB, stopping the cascade to dementia before it
can start or gain momentum.
For more on the role that a "leaky" BBB might play
in AD and other forms of dementia, see "Holes in the
Shield" by D. Kaufer and A. Friedman, Scientific
American, 05/2021, from which this image is
taken.
Setting aside the positive effects of
these drugs, it's also the case that pharmacotherapy
has some problems:
In many instances, the drugs just don't work. A large
portion of patients for whom antidepressant drugs are
prescribed do not respond to them fully, so their
depression never really lifts. In other cases, the
patients will relapse into depression even though they
remain on a drug that seemed to work at first.
It is not easy to predict which of the available drugs
will work for a particular patient. The result is that
many patients must go through an extended period of
"adjusting their medication" until their therapist
stumbles on the one that works for them. If depression
were simply a matter of making more serotonin (or
norepinephrine) available at the synapse, we would expect
all of the antidepressant drugs to have pretty much the
same effect.
Many medications have undesirable side effects, such as
the "Parkinsonism" (mimicking the symptoms of Parkinson's
disease) and tardive dyskinesia that frequently
accompanies the use of antipsychotic medications.
There is a certain lack of specificity in the actions of
drugs -- as when Paxil, an SSRI, is used to treat anxiety
as well as depression.
Along these lines, there is good evidence that the
effects of many psychiatric drugs, including the SSRIs,
are heavily loaded with placebo effects. According to one
estimate, fully 75% of the effect of antidepressant
medication is attributable to placebo, rather than any
specific pharmacological action.
Link
to a segment of60 Minutes,
interviewing Prof. Irving Kirsch and others on placebo
effects in the drug treatment of depression, broadcast
on CBS 02/19/2012.
But that doesn't mean that antidepressants are just
placebos. There is good evidence that they are
especially effective for patients with severe or very
severe episodes of depression -- less so in patients with
mild to moderate depression (Fournier et al., 2010).
Patients with mild to moderate depression may be
helped just as much, if not more, by psychotherapy as
opposed to medication.
Psychiatric drugs provide symptom relief, but they do
not provide a cure, in the sense of reversing underlying
biological and psychological deficits. Patients on
medication will often relapse if their medication is
discontinued/
The prospects of relapse are likely to be diminished if
medication is combined with psychotherapy (see below).
On the other hand, there is some evidence that
medication can actually interfere with
psychotherapy (Forand et al., 2013).
The Great Antidepressant Debate
Antidepressants are probably the most commonly
employed psychiatric medications, but the last 10
years or so has seen a vigorous debate over their
actual effectiveness. The bottom line is that
they are effective, but there are also some
caveats.
What might be called "the Great
Antidepressant Debate" began with a
provocative article by Kirsch and Sapirstein
(1998) entitled "Listening to Prozac But Hearing
Placebo". K&S conducted a
meta-analysis of 19 published studies in
which an antidepressant medication (such
as Prozac) was compared to placebo.
They found that
the median effect size
(D)
for the drug groups was 1.55 standard
deviations (SDs), compared to D = 0.37
for the untreated controls,
which
sounds pretty good -- until they found that D
for the placebo was 1.16
SDs -- approaching the value
obtained for the patients who received the
active drugs. On the
basis of their results, K&S concluded that spontaneous
remission (natural
history) accounted for about 24%
(.37/1.55), while placebo accounted
for approximately 51% ((1.16 -
.37)/1.55); their conclusion, then was
that the active ingredients in antidepressant
medications accounted for only about 25% of
the outcome in the drug
treatment of depression (100-24-51).
As you might imagine,
this claim drove psychiatrists, who
generally favor drugs over
psychotherapy, and even some
psychologists (who sometimes envy
psychiatrists' ability to prescribe
drugs), quite crazy. Kirsch's
title was, in fact, a deliberate play
on Listening to Prozac (1993), a pean to
the drug by psychiatrist Peter
D. Kramer.
But wait,
there's more.
K&S relied on
published clinical
trials, but it is well
known that both
scientists and
scientific publication
favors positive over
negative results.
If you've got a new
drug, nobody cares if it
doesn't
work.
Pharmaceutical
companies, who finance
the vast bulk of
research on psychiatric
medications, conduct a
lot of studies during
the drug-development
process, but all the
Food and Drug
Administration cares
about is that there are
at least two independent
studies showing that the
new drug is
significantly better
than placebo. So
there might be lots of
unpublished studies
where the drug didn't
prove to be better than
placebo -- what is known
in the trade as the file-drawer
problem.
Fortunately,
while the drug companies
don't have to submit
negative results to the
FDA, they do have to
register all trials in
order to secure eventual
FDA approval. Turner
et al. (New England
Journal of Medicine,
2008) obtained the results
of these trials, involving
12 different
antidepressant drugs,
through the Freedom of
Information Act
(FOIA). Of the 74
registered studies.
Half of
these studies (37/74)
were published, and
all of them reported
positive outcomes;
only 1 positive study
was unpublished.
Of the
remaining 36 studies,
22 were not published
at all, and another 11
were published in such
a way as to obscure
the negative findings;
only 3 negative
studies actually saw
publication. So
there is a clear
positivity bias in
publication.
Based on
the 51 published
studies, the overall
effect size for the
antidepressant drugs
was .37 (Hedges' g),
which is interpreted
as a small-to-moderate
effect.
But if
you pooled all 74
studies together, the
overall effect size
for the drugs fell to
g = .15, which
doesn't even qualify
as a small
effect.
In addition
to revealing a tendency
toward selective
reporting on the part of
researchers (and the
drug companies who
supported them), the
Turner study suggests
that, all things
considered,
antidepressant
medications might be
less effective than
would be apparent from
the published studies
alone. Now, there
are a lot of reasons
that studies don't get
published, and some of
the negative studies
might have been poorly
designed or
executed. But
still, there's a bias in
the publication system
that potentially
exaggerates the
effectiveness of these
drugs (and probably
other drugs as well --
and not just psychiatric
ones!).
At the same time, Kirsch et al. (PLoS,
2008) examined many of these studies, both published
and unpublished (thanks again, FOIA!) from a
different perspective. The FDA standards
require only that the new drug be significantly
better than placebo; but, as we'll discuss again
later, there is a big difference between a statistically
significant difference and a clinically
significant one. With a large-enough N,
even very small differences become statistically
significant; and these changes may be too small to
result in any real change in the patient's
status. In the studies reviewed by Kirsch et
al., the average difference between the drug and
placebo groups on the chief outcome measure,
improvement on the Hamilton Rating Scale of
Depression, was less than 2 points. This is
statistically significant, given the more than 5,000
patients involved. But that figure was below
the minimum of 3 points established by the National
Institute of Clinical Excellence, a British group,
for a clinically significant difference. The
drug-placebo difference was greatest for those
patients with more severe levels of depression.
Reviewing the 2008 Turner et al. and Kirsch et al.
studies, Ioannidis (2008) concluded that "the use of
many small randomized trials with clinically
non-relevant outcomes, improper interpretation
of statistical significance, manipulated study
design, biased selection of study populations, short
follow-up, and selective and distorted reporting of
results has built and nourished a seemingly
evidence-based myth on antidepressant
effectiveness", and suggested that "higher evidence
standards, with very large long-term trials and
careful prospective meta-analyses of
individual-level data may reach closer to the truth
and clinically useful evidence".
Kirsch
presented additional
analyses in a
book, The Emperor's
New Drugs: Exploding the
Antidepressant
Myth (2011), that was
highly critical of the
use of
antidepressants. In
response, Kramer recently
published a new book, Ordinarily
Well: The Case for
Antidepressants
(2016), which conceded
that antidepressant
medication works best
for the most severely
depressed
patients, but argues that
a combination of
medication and
psychotherapy is good for
everyone.
In the latest
salvo in this ongoing
dispute, Cipriani et al.
(2018) performed a
meta-analysis of an
expanded set of more than
500 published and
unpublished clinical
trials of antidepressant
medication, involving more
than 100,000 patients
receiving 21 different
first- and
second-generation
antidepressant medications
(or placebo). All
the drugs proved to be
more effective than
placebo, though
head-to-head comparisons
showed that some drugs
were, on average, more
effective than
others. In the
drug-placebo comparisons,
the average effect size
was characterized as
"modest".
The point
of all this is not to
diminish the value of
antidepressants: a
modest effect is not
nothing. The
meta-analyses are
convincing, but Kramer's
response is probably
correct: when people are
depressed, the
combination of drugs and
psychotherapy can be
very helpful. The
point is that even
powerful psychoactive
drugs have substantial
placebo components, and
this is likely
to be true for the
major and minor
psychedelics as
well. As
Kirsch et al. (2002)
point out, "Placebo
alcohol produces
effects that are not
observed when
alcohol is
administered
surreptitiously...".
.
Perhaps the most important consequence
of the pharmaceutical revolution in mental health has been to
give practitioners, and therapists, a means for managing
chronic mental illnesses. In this way, the pharmacological
treatment of major mental illness is analogous to the use of
insulin to treat diabetes. Patients with schizophrenia will
still have schizophrenia, and patients with depression will
still have depression, but with medication they can better
deal with their illnesses, and lead more productive lives.
That's a nontrivial benefit, but genuine cures for mental
illness are going to have to wait for further pharmaceutical
advances -- or, perhaps, another approach entirely.
Clinical Trials
Pharmaceutical companies can't just market any old
drug for any old purpose. In the United States, the
Food and Drug Administration (FDA) must approve
specific formulations for specific purposes, with
specific warnings about contraindications and
side-effects, based on research known as a clinical
trial. Clinical trials take place across
a sequence of several phases:
Preclinical Research, including the
discovery of a new pharmaceutical compound,
development of large-scale manufacturing
capability, and testing on nonhuman animals.
Phase I Clinical Trials, small-scale
human studies on healthy non-patients, intended to
establish the maximum dose of the drug that is
safe to administer.
Phase II Clinical Trials, larger-scale
pilot studies of actual patients (e.g.,
individuals carrying a diagnosis of major
depressive disorder), intended to establish "end
points" (dependent variables, e.g., reduction in
scores on a depression scale), provide estimates
of effective doses and duration of treatment, and
determine what kinds of patients (e.g., mild,
moderate, or severe depression) should receive the
drug.
Phase III Clinical Trials, full-fledged
efficacy studies involving very large numbers of
patients, intended to establish both clinical
efficacy and reveal important side-effects of
treatment.
Phase IV Clinical Trials constitute
continued research, after a new drug has been
approved, licensed, and marketed, to refine the
standards for its use.
Typically, the FDA requires two separate trials
showing a statistically significant difference
between treatment with the investigational new
drug (IND) and placebo. Sometimes
the IND is compared to the standard of care
-- which is often an older drug. Only about 20% of
IND applications result in actual approval by the
FDA
In meeting the FDA standards, it does not matter
how many failed trials have been conducted -- that
is, trials which fail to yield a significant
difference between the IND and placebo. Given
the standard of p < .05, meaning that a
statistically significant difference between two
conditions would be expected to occur less than 5
times out of 100 just by chance, in principle this
means that a pharmaceutical company could conduct as
many as 50 or 100 studies, and just report the
studies that happened to yield significant results just
by chance! In fact, something like this
seems to have happened in the case of some
antidepressants: some pharmaceutical companies
reported only the results of positive trials -- a
phenomenon known as the file drawer problem
(for more details, see The Emperor's New Drugs
by Irving Kirsch). In other cases, the company
will conduct a meta-analysis, combining many
small trials, only some of which have yielded a
statistically significant result, into a much larger
study that shows an overall positive effect.
For this reason, the FDA now requires drug companies
to register all their clinical trials in advance, so
it can be determined how many negative studies were
left "in the file drawer".
After the Phase III clinical trial has been
successfully concluded, and the drug has been
approved for use, research still isn't done.
FDA review and approval is then followed by post-marketing
surveillance intended to identify additional
adverse reactions, other side-effects, and
contraindications that did not show up during the
formal clinical trials. This information may result
in withdrawal of FDA approval, or a requirement to
provide additional warnings or other information on
the drug's label.
A similar sequence of clinical trials is required
for the approval of non-pharmaceutical treatments,
such as heart pacemakers, or new surgical
techniques.
No research at all is required for the marketing
of herbal remedies, such as St. John's Wort.
This is because these substances occur naturally, in
nature, and are classified as "foods" rather than
"drugs". For this reason, herbal remedies are
often marketed with no, or very poor, research to
back up the marketer's claims.
Once a pharmaceutical firm has developed a drug,
the clinical trials have to be run by physicians
with patients who might benefit from them.
Unfortunately, there are often strong financial ties
between these physicians and the drug companies --
ties that are so strong that they might bias the
physicians' evaluations of the drugs. To help
allay this problem, in 2013 Congress passed the
"Physician Payments Sunshine Act", which requires
pharmaceutical firms and medical-device
manufacturers to disclose most of their financial
relationships with the physicians who perform
research for them -- most, that is, but not
all.
For more details, see "Understanding Clinical
Trials" by Justin A. Zivin, Scientific
American, April 2000). See also "Is
Drug Research Trustworthy?" by Charles Seife (Scientific
American, 12/2012), which discusses in
detail the problem of financial ties between
pharmaceutical companies and the medical
researchers who actually perform clinical trials.
The Life History of a Psychotropic Drug
The process of drug approval can take years and be
very expensive. Consider the example of
Cymbalta, a popular SSRI (as described by Sarah
Amandolare in "Life of a Drug", Scientific
American Mind, September-October 2013).
In the early 1950s, researchers discovered that
iproniazid, a drug used in the treatment of
tuberculosis, also had positive effects on
patients' mood.
Pharmacologists also discovered that iproniazid
had specific effects on serotonin, norepinephrine,
and dopamine.
In 1974, researchers working at Eli Lilly
developed fluoxetine, the first SSRI, which was
later marketed as Prozac.
In the 1980s, researchers started trying to
develop SNRIs as well -- including duloxetine,
which inhibited the reuptake of norepinephrine as
well as serotonin, later to be marketed as Cymbalta.
Eli Lilly applied for a patent for duloxetine
(not yet known by its trade name of Cymbalta) in
1986, and received it in 1990.
Only at that point could Eli Lilly begin Phase I
clinical trials. these were concluded in
2000.
In 2001, Eli Lilly applied for FDA approval of
Cymbalta. This application was unsuccessful,
requiring the company to engage in additional
Phase I and Phase II trials
In 2003, the FDA again denied approval of the
drug, citing (among other problems) liver disease
as a potential side effect..
Eli Lilly completed additional Phase III
clinical trials.
Finally, in 2004, the FDA approved Cymbalta for
the treatment of depression, enabling the company
to market the drug for that purpose..
Post-marketing surveillance continues, as well
as new clinical trials aimed at other
disorders. But...
Eli Lilly's patent on duloxetine, originally
received in 1990, will expire in 2013, enabling
other manufacturers to offer generic
versions of the drug. At that point,
Cymbalta will no longer be particularly
profitable, and the the company may be forced to
lay off employees who have been working on this
particular drug -- or assign them to new duties
developing and studying new INDs.
Psychotropic Medication: A Guide for the
Prospective Consumer
Prof. F. Scott Kraly, author of Brain Science
and Psychological Disorders: New Perspectives on
Psychotherapeutic Treatment (2006), offers the
following questions for those who are considering a
prescription for psychotropic medication:
When You Are the Patient:
Given my diagnosis, is psychotropic medication
necessary, or would counseling or psychotherapy
be as, or more, effective?
Is there published scientific evidence that
supports the use of this mediation for my
diagnosis? If not, what is the
justification for going off-label?
What percentage of patients using this
medication are likely to benefit?
If this medication does not improve my
symptoms, or if I find the side effects
intolerable, what is the alternative plan for my
treatment?
What are the most likely side effects?
When can I expect to stop using the
medication? When that day comes, what will
I be advised to do to avoid a relapse?
What can I read to better understand my
situation?
And, ask yourself these questions:
Now that I've been advised on exactly how to
use the drug, will I be committed to follow
those instructions faithfully? (If not,
why am I being a bad patient?)
Does the drug produce a side effect that I
might find so intolerable that I would quit
using it, or ask my doctor to prescribe a
different medication?
When your child is the patient
Given the diagnosis, is it absolutely
necessary and in the best interests of our child
to expose his/her brain to a drug? Might
behavior therapy or psychotherapy be a
reasonable alternative?
Can the duration of time our child uses
medication be shortened if we support the drug
therapy with behavior therapy or psychotherapy?
Is there published scientific evidence from
clinical trials in children that supports the
use of this medication for this diagnosis?
If not, what is the justification for the
off-label prescription?
What potential drug-induced side effects
should we be vigilant about detecting?
What questions should we ask our child
regarding his or her feelings abut the drug's
effectiveness or side effects?
Keep in mind the factors and principles of
pharmacology that can determine the effectiveness
of drug therapy:
No drug has only one effect; side effects are
inevitable.
Compromise on benefits and risks is a
realistic goal.
Psychotropic medication is often best used
together with psychotherapy.
The main effects and side effects of a drug
depend upon the dosage.
Age, sex, genetics, drug history, and
ethnicity can affect effectiveness.
A drug can have enduring effects upon the
brain.
A drug can alter the development of a young,
maturing brain.
The FDA cannot ensure that a drug will be
effective and safe for every individual.
Herbal remedies and dietary supplements may
not be effective or safe.
Off-label usage of a drug is not based upon
scientific evidence.
Avoid polypharmacy, if possible, because some
drug interactions can be potent, unpredictable,
and harmful.
But Just Because He Takes Zoloft...
...doesn't mean that he's depressed. Zoloft
is a powerful SSRI antidepressant; but, like all
drugs, it can be prescribed for purposes other than
the treatment of depression. For example, some
antidepressants are also effective in the treatment
of migraine headaches. So you can't diagnose
"backwards", inferring from a drug that someone
takes what mental illness he might have. He
might not have any. So, the next time you're
rummaging around in someone's medicine cabinet,
don't jump to hasty conclusions!
The FDA approves drugs for certain conditions,
based on the results of controlled clinical trials,
and these indications are indicated on the drug's
label. But for a variety of reasons,
physicians can also prescribe drugs "off-label".
There may be good evidence that a drug is
effective for a certain condition, even though the
required clinical trials have not yet been
completed. Clinical trials can cost a lot of
money, and sometimes pharmaceutical companies
simply don't want to make the investment.
There may be no FDA-approved drug for a
particular treatment.
No approved drug is effective in a particular
instance.
A drug may be prescribed for children, even
though it has not been approved by the FDA for use
in young patients.
For more information, see "The Unadvertised
Uses of Drugs", Scientific American Mind,
may-June 2013.
Psychotherapy
Pharmacotherapy
is a relatively new approach to the treatment of mental
illness. Historically, the active treatment of mental illness
was limited to various forms of psychotherapy, a
"talking cure" in which a therapist engaged in activities that
were intended to change the contents of the patient's mind: to
alter patients' beliefs, feelings, desires -- and thus their
behavior. Although there were important precursors, the birth
of psychotherapy is commonly given as 1893, when Sigmund Freud
and Joseph Breuer began publishing the articles that were
eventually collected as their Studies in Hysteria.
Pharmacotherapy attempts to alter mental
functions indirectly, by altering the chemistry of the
brain.
Psychotherapy attempts to alter the mind
directly, through various sorts of learning experiences.
There are literally
hundreds of different psychotherapies, but they can all be
classified under three major headings:
Psychodynamic,
Insight-Oriented Psychotherapy, such as Freudian
psychoanalysis. In this technique, the therapist helps the
patient gain insight into unconscious conflicts that
presumably lie at the root of his or her symptoms. For
Freud, these conflicts involved primitive, unconscious
sexual and aggressive urges, which gave rise to anxiety,
which the patient reduced by engaging in repression and
other psychological defenses, which in turn caused
symptoms to occur. Psychoanalysis was intended to help the
patient become aware of these conflicts, and acknowledge
his primitive urges, so that the defenses would no longer
be needed and the symptoms would disappear.
"Neo-Freudian" psychoanalysis retained the emphasis on
unconscious conflict, but de-emphasized biological
drives having to do with sex and aggression, and focused
instead on conflicts the patient encountered in the
"real world". Classic psychoanalysis was a
5-times-per-week affair; what is known as psychoanalytic
psychotherapy is less intense, but follows much
the same rationale as the classic form.
Behavior Therapy began in the 1950s as a
behavioristic reaction to the "mentalism" of
psychoanalysis. Rather than resolving the unconscious
conflicts that supposedly underlay the patient's symptoms,
behavior therapists like Joseph Wolpe sought to modify the
symptoms themselves, directly, by means of techniques
derived from learning theory. From their point of view,
symptoms were not caused by disease; rather, the
symptoms were the disease. In some cases, such as
phobias and obsessive-compulsive behaviors, the assumption
was that the symptoms were learned behaviors that could be
unlearned; even if the symptoms were not acquired through
learning, however, it was assumed that they could be
modified by learning (some forms of behavior therapy were
called behavior modification).
Cognitive Therapy: Later, in the aftermath of
the "cognitive revolution" in psychology, which
supplanted behaviorism,behavior therapy was
supplanted by a cognitive therapy which
attempted to alter the patient's behaviors, whether
overt or covert), by changing the patient's
cognitions; early proponents of cognitive therapy were
Aaron (Tim) Beck, known for his cognitive theory of
depression, and Albert Ellis who practiced what he
called rational-emotive psychotherapy. In
2006, Beck received the prestigious Lasker Award for
clinical research -- the first ever given to a
psychiatrist for research on treatment. The chairman
of the award jury noted that cognitive therapy "is one
of the most important advances -- if not the most
important advance -- in the treatment of mental
diseases in the last 50 years" (New York Times,
09/17/06).
Cognitive-Behavioral Therapy: Even with the
new "mentalism" of cognitive psychology, the goal of
cognitive therapy was to change the patient's
behavior, so the hybrid term cognitive-behavioral
therapy (CBT) became popular. Whereas
psychodynamic therapy focuses on the patient's past,
especially his childhood, CBT focuses on the "here and
now" of the patient's life.
Humanistic
Psychotherapy emerged as a reaction to both
psychoanalysis and behavior therapy. In both kinds of
therapy, the therapist was extremely directive; but --
either keeping the patient focused on unconscious
conflicts, or Both , which were perceived as much too
directive. Carl Rogers introduced a client-centered
therapy in which the patient set the therapeutic
agenda, and the therapist helped create an environment
of unconditional positive regard in which the
patient could achieve self-actualization (a term
introduced by another humanistic psychologist, Abraham
Maslow). Rogers' language is very revealing here:
"patients" are passive recipients of the action of
"agents"; but "clients" hire people, like lawyers, to
work for them.
Psychodynamic Psychotherapy
Contemporary
psychodynamic psychotherapy has its origins in classical
Freudian psychoanalysis. But just as "neo-Freudian" theories
of personality were de-biologized and de-sexualized, so has
contemporary psychodynamic psychotherapy.
Jonathan Shedler (2010) has summarized
the main principles of contemporary psychodynamic
psychotherapy as follows:
Focus on the experience, expression, and discussion of
emotion (in contrast to the focus of cognitive-behavioral
therapy on thoughts and behaviors).
Exploration of the patient's attempts to avoid, resist,
and defend against distressing thoughts and feelings.
Identification of recurring themes and patterns in the
patient's relationships.
Discussion of past experiences, especially the
ostensibly formative experiences of childhood.
Focus on interpersonal relations and attachments.
Focus on the therapeutic relationship between patient
and therapist, which may reflect repetitive themes in the
patient's relationships with others outside of therapy.
Exploration of fantasy life, including dreams and
fantasies, but generally allowing the patient to give free
expression to whatever is on their minds, instead of
following an agenda set by the therapist.
Shedler points out that modern
psychodynamic therapy, while rooted in Freud, has shed most of
the trappings of classical psychoanalysis. There is
little attention paid to the Oedipus conflict and castration
anxiety, for example1 Patients don't necessarily lie on
a couch and free associate for 50 minutes a session, five
sessions per week. Rather, modern psychodynamic
psychotherapy is practiced as an open-ended vehicle for
self-examination -- which means that it might be useful even
for people who don't suffer from depression, anxiety, or some
other form of mental illness.
For a first-person account by a writer who spent most of her
adult lifetime (and, for that matter, a considerable amount of
her childhood) in psychoanalysis, see "My Life in Therapy" by
Daphne Merkin (New York Times Magazine, 08/08/2010) --
or, for a longer treatment,Mockingbird Years: A Life In and
Out of Therapy (2000), a book-length memoir from Emily
Fox Gordon. For some patients in long-term psychodynamic
psychotherapy (and here we think of Woody Allen), the
treatment -- especially if it includes hospitalization at an
institution like Austen Riggs, or the MacLean Hospital, or the
Menninger Clinic -- takes on a kind of Romantic feeling, not
unlike the tuberculosis sanitarium depicted in Thomas Mann's
novel,The Magic Mountain.
Cognitive-Behavioral Therapy
Especially where maladaptive social
learning lies at the heart of the patient's illness,
psychotherapy can achieve a full-fledged cure through what are
essentially re-education techniques -- that is, by arranging
new learning experiences that undo, or modify, the effects of
old ones. Even when the patient's symptoms are not acquired
through learning, at least in the usual sense,
cognitive-behavioral therapy can help patients to acquire new
modes of thought, and new behaviors, that will counteract the
effects of their illness.
Exposure Therapies
Cognitive-behavioral
therapy was first introduced for the treatment of anxiety
disorders, especially phobias and obsessive-compulsive
disorder. Among the most popular techniques of CBT are:
Systematic Desensitization, involving a
progressive, graded exposure to a phobic stimulus; and
Flooding, also known as Implosion Therapy
(there are technical differences between these), in which
the patient is immediately immersed in the most
frightening situation -- either direct contact with the
phobic object, or rehearsal of an obsessive thought and
prevention of compulsive behavior.
In both cases, the patient can
experience complete alleviation of anxiety, which will never
return -- the very definition of a cure -- through the
extinction of fear, aversion, or other response, and the
acquisition of more appropriate, adaptive behaviors. In the
treatment of phobias, systematic desensitization and flooding
are equally effective. Flooding is more efficient, but it is
also somewhat more dangerous: if done improperly, the patient
will be left worse off than when he started, so don't try
this at home.
Relaxation Therapies
For
the psychophysiological (psychosomatic) disorders, the best
treatment is to eliminate the stressor from the patient's
environment. However, this is not always possible, in which
case the therapy involves modifying the patient's response,
including physiological responses mediated by the autonomic
nervous system, to the stressor.
Relaxation Training seeks to achieve a general
reduction in the patient's emotional reaction to the
stressor, essentially modulating the general
adaptation syndrome (see the lecture supplements on
the Biological Bases of Mind and Behavior).
Biofeedback permits the patient to gain some
voluntary control over the functioning of some element of
the autonomic nervous system, such as heart rate or blood
pressure. Because ANS activity is not accessible to
conscious awareness, the therapist must use special
physiological monitoring devices, such as the EKG or EMG,
to provide information to the patient about his or her
internal physiological state. In biofeedback, the
apparatus signals the patient's level of physiological
activity, and the patient learns, through a feedback
process similar to instrumental conditioning, to control
his own physiological state.
Cognitive Restructuring
Other
aspects of mental illness, particularly anxiety,depression,
and the delusions of schizophrenia and bipolar
disorder, appear to reflect maladaptive knowledge or belief
acquired through learning.
According to Beck's original cognitive theory,
depression is caused by a particular set of beliefs, as
well as a cognitive style that maintains those beliefs.
Similarly, following the learned helplessness model of
Seligman, Abramson, and Alloy, depression may be caused by
the patient's belief that important, particularly aversive
events, are uncontrollable.
Similarly, anxiety may be caused by the patient's belief
that such events are unpredictable.
Delusions may reflect the patient's inappropriate
attempts to explain the anomalous experiences associated
with schizophrenia and the manic-depressive mood swings of
bipolar disorder.
In these cases, the goal
of cognitive therapy is to change the patient's underlying
cognitive structures, or schemata:
Confront the patient with schema-incongruent information
that will stimulate schema change.
Provide a more adaptive way of construing the patient
him- or herself, others, various social situations, the
past, present, and future;
Change the patient's interpretation of the situation,
and construal of experience;
Alter the patient's expectations of the future.
Beck's cognitive therapy for depression
entails altering the patient's depressogenic schemata
-- the "depressogenic triad" of negative beliefs concerning
oneself, the world, and the future. Cognitive therapy also
seeks to alter the patient's tendency toward arbitrary
inference, selective abstraction, overgeneralization,
magnification, and minimization that maintain these schemata
once established.
Based on the learned helplessness
theory of depression, Seligman, Abramson, Alloy, and their
colleagues have suggested that depression may be alleviated by
changing the individual's "depressogenic" attributional style
that leads to feelings of helplessness and hopelessness, so
that the patient will make more realistic, adaptive causal
attributions about events.
CBT for Insomnia
A good example of how behavioral
and cognitive therapy can be combined is Cognitive-Behavioral
Therapy for Insomnia
(CBT-I). I go into detail
on this treatment because sleep is such an issue for
college students -- and for so many other people, too.
CBT-I has five major components:
Stimulus Control: Strengthening the
association between the bed and sleeping.
Go to bed only when you are actually tired.
Do nothing in bed except sleep and have sex.
Get out of bed at the same time every morning.
If you do not fall asleep within 10 minutes of
going to bed, get up, move to another room, and do
something relaxing until you feel sleepy.
Sleep Hygiene: Altering the environment to
make it more conducive to sleep.
Within 4 to 6 hours of going to bed, limit the
intake of substances such as caffeine, nicotine,
and alcohol that interfere with sleep.
Take a light snack, such as milk or peanut
butter, instead.
Avoid stimulating activity prior to sleep
Get rid of all distractions: No TV, no
computer games; Turn off the cell phone!
Read a book, write an e-mail, take a warm
bath.
Sleep Restriction:Control the time
you spend in bed, to maximize "sleep efficiency" and
restore "sleep homeostasis" -- that is, the
biological need to sleep.
Sleep Efficiency (SE) = Total Sleep Time (TST) /
Time in Bed (TIB), with the ratio expressed as a
percentage.
Increase TIB if SE > 90%
Decrease TIB if SE < 80%
Sleep Restriction involves paradoxical
intention, a concept first articulated by
Viktor Frankl, founder of existential psychiatry,
in 1959. It also played a prominent role in
the techniques of an American maverick
psychotherapist, Milton Erickson, as detailed by
an early disciple, Jay Haley (Strategies of
Psychotherapy, 1963; Uncommon therapy,
1973).
Relaxation Training is a set of techniques,
imported from systematic desensitization and
stress-reduction therapies, intended to promote
physical relaxation.
Cognitive Therapy includes educating the
patient about sleep, changing any dysfunctional
attitudes or beliefs that the patient may have about
sleep, and controlling the patient's worries about
losing sleep.
Social Skills Training
Many behavioral disorders and
annoying problems in living often result from the
individual's inadequate social skills. Public-speaking anxiety, while not necessarily rising
to the level of a full-fledged social phobia, can be extremely
debilitating, but can be relieved simply by giving the person
practice in public speaking in a controlled, friendly
environment. Many people have a great deal of trouble saying
"no" to people, including their parents (or children) or
spouses. In this case,assertiveness training can help
people make, and respond to, demands more adaptively. People's
sexual problems are not limited to impotence or frigidity.
Often, the difficulties that people have in maintaining sexual
arousal, or achieving orgasm (in oneself or one's partner)
reflects a simple lack of knowledge about how to make love
(sex is a biological function, and in that sense natural, but
the pleasure-giving and -receiving aspects of lovemaking don't
come naturally -- as almost anyone who remembers his or her
first sexual experiences can attest. Many people learn to make
love through practice, but many people need instruction in the
form of sex therapy -- not necessarily from a sexual
surrogate, but sometimes just some friendly advice.
Cognitive-Behavioral Therapy and Social
Intelligence
Whereas pharmacotherapy attempts to
alter the disordered mind by altering the chemistry of the
brain, psychotherapy attempts to alter the disordered mind
directly through learning experiences.
Much of cognitive-behavioral therapy
seeks to alter the patient's declarative knowledge
about what to believe and expect in various situations, social
skills training, like relaxation training and biofeedback,
seeks to alter the patient's procedural knowledge
about what to do in those situations. Taken together, the
cognitive-behavioral therapies work by altering the
individual's social intelligence -- his or her fund of
knowledge about self and others, and repertoire of
interpersonal skills -- that he or she uses to navigate in the
social world (see the lecture supplement on Personality and
Social Interaction).
Outcomes of Psychotherapy
The
notion of psychotherapy is fine in principle, and it's made a
healthy living for several generations of psychiatrists,
clinical psychologists, clinical social workers, and other
mental health professionals. But does it really work?
Psychotherapy is plagued by what might be called the Woody
Allen Bugaboo -- after the characters played by the
actor-director, who go through years, decades, of
psychoanalysis but never seem to change.
In fact, psychotherapy came to a crisis
in the 1950s when Hans Eysenck, a British psychologist,
reviewed the literature and claimed that psychotherapy was
ineffective -- that people who received psychotherapy had no
better outcomes than those who received no treatment at all.
Along with the evident success of pharmacotherapy, and
lingering doubts such as expressed by the Woody Allen Bugaboo,
therapists were challenged to demonstrate, scientifically,
that psychotherapy really helps people with mental illness.
Since
Eysenck's original study, a large body of empirical research
shows that, contrary to his conclusions, psychotherapy can be
an effective treatment for mental illness. For example, a
classic study by Smith, Glass, and Miller (1980) employed a
technique called meta-analysis (see the lecture
supplement on Statistics and Methods) to combine the results
of a large number of studies that compared adult patients who
received various forms of psychotherapy to control patients
who were untreated. Quantifying psychotherapy outcome isn't
easy, but it can be done, and it's necessary if we're going to
analyze the effects of psychotherapy statistically. Typically,
the control patients were not denied treatment, but were
merely put on a "waiting list" until a therapist became
available. So, the question can be reformulated along these
lines: given X months or years since their diagnosis, have
patients who received psychotherapy improved more than those
who did not? The answer is yes: in the Smith et al. analysis,
that the median patient receiving psychotherapy did better
than about 75% of the control patients.
Another finding of the Smith et al. study
was that patients who received psychotherapy did better than
those who did not, regardless of what form of therapy they
received. This finding led some commentators to conclude that
all forms of therapy are equivalent. It doesn't matter what
the therapist does, so long as the patient sees one.
Saul Rosenzweig (1937) an early leader clinical psychology,
has expressed this point of view as the Dodo Bird Verdict,
after an episode in Lewis Carroll's Alice's Adventures in
Wonderland (1865). Lester Luborsky (1975), a
psychoanalyst and prominent psychotherapy researcher at the
University of Pennsylvania, popularized the term.
When Alice discovered that she would not get
out of the rabbit hole, she was engulfed in a pond of her
own tears, which also drenched a number of animals, such as
The Mouse. The Dodo Bird suggested that the animals run a
Caucus Race to get dry. The animals ran around until they
ran out of breath and stopped. When Alice asked who had won
the Caucus Race, the Dodo Bird replied that "everyone has
won and all must have prizes".
The Dodo Bird verdict has been a source
of comfort to some psychotherapists who prefer to use those
psychodynamic forms of therapy that have come under attack by
modern scientific psychology, as well as those who believe
that the therapeutic relationship between therapist and
patient is more important than anything the therapist does
(e.g., Frank, 1961; Wampold, 1997, 2001)). Put another way,
the "tie-score effect" is taken as indicating that the various
forms of therapy have more in common than appears on the
surface (see, for example, the Great Psychotherapy Debate:
Models, Methods, and Findings by Bruce E. Wampold,
2001). But the Dodo Bird Verdict is troubling, too, because is
suggests that the effects of psychotherapy are nonspecific --
that is, that there is no particular "active ingredient" that
makes therapy effective. Put another way, it suggests that
psychotherapy is simply a kind of placebo. And since
psychiatric medications are approved for use precisely because
they have been shown to be better than placebo, that suggests
that psychotherapy is inferior to pharmacotherapy.
Fortunately, the Smith et al. study
contained an analysis that showed that the Dodo Bird Verdict
is not quite right: some psychotherapies work better than
others. This is already evident in the data presented earlier,
which showed that patients who received cognitive-behavioral
forms of therapy did even better, compared to controls, than
patients who received psychodynamic or humanistic forms of
therapy. To examine this issue further, Smith et al. computed
measures of effect size (see the lecture supplement on
Methods and Statistics) for each of the studies included in
their analysis.
The effect size d is a measure of the
difference in mean outcomes between two treatments,
expressed in standard deviation units. Thus, an effect size
of 1.0 means that the average subject in the experimental
group scored 1 standard deviation higher than the average
subject in the control group. According to Cohen (1977),
effect sizes in behavioral and social research can be
classified as follows:
d = .20: a small effect;
d = .50: a moderate effect;
d = .80: a large effect.
When
Smith et al. calculated the average effect size for different
types of therapies, all forms of therapy were shown to have at
least moderate-sized effects, consistent with the Dodo Bird
Verdict. However, the effect sizes associated with the
cognitive and behavioral therapies were much larger than those
associated with the psychodynamic and humanistic forms.
In the Smith et al. meta-analysis, the
effect of psychotherapy overall, without regard to the form of
therapy or the condition being treated, was quantified as an
"effect size" of 0.85 -- which is generally considered a
"large" effect in medical, psychological, and social-science
research.
A later review by Lipsey and Wilson
(1993) -- actually, a mega-analysis, or meta-analysis
of published meta-analyses (18 in all), obtained a median
effect size of .75 -- which is a substantial effect by any
standard.
Similar
results were obtained in a meta-analysis of psychotherapy for
children and adolescents by Weiss and Weisz (1995).
Other studies have also demonstrated the
general superiority of cognitive-behavioral therapies:
Chambless and Ollendick (2001) reviewed studies of
treatment of the anxiety disorders, and also of depression
and behavior problems in children and adolescents.
Tolin (2010) reviewed studies of the treatment of
anxiety and mood disorders.
Based on these studies, and others like
them, it appears that all psychotherapies are not created
equal: as a rule, cognitive and behavioral therapies are more
effective than psychodynamic and humanistic therapies.
Other considerations also
suggest that the Dodo Bird Verdict is wrong:
For specific illnesses, some forms of therapy are more
effective than others: in general the cognitive and
behavioral disorders are more effective than
insight-oriented therapies in the treatment of a wide
variety of mental illnesses, especially the anxiety
disorders.
Moreover, the cognitive-behavioral therapies are more
efficient than the insight therapies, achieving their
results in less time, and therefore with less expense to
the patient or insurance companies.
And some forms of therapy may even be harmful. For
example, crisis debriefing does not appear to help
patients suffering from post-traumatic stress disorder,
and may even make their problems worse.
Therapies can be harmful when they are based on the
wrong theory of illness -- as, for example, when a
patient's symptoms are attributed to "repressed
memories" of childhood sexual abuse.
For that reason, cognitive-behavioral
treatments are quickly emerging as the "standard of care" in
the psychological treatment of mental illness and problems in
living.
This does not mean, however, that
psychodynamic psychotherapy is not effective. Although
classical psychoanalysis, which is what Eysenck studied in the
1950s, does not seem to be more effective than no treatment,
better results have been obtained with contemporary forms of
psychodynamic therapy.
For example, Shedler (2010) cited a
2006 meta-analysis of psychodynamic therapy that yielded an
overall effect size of 0.97.
The real question, though,
is not the comparison of overall effect sizes. Questions about
the efficacy of psychotherapy are better framed more
specifically:
What kind of treatment works best for each particular
disorder?
And when two different treatments are effective, which
one is more efficient, and less expensive?
What are the particular mechanisms by which a treatment
achieves its successful outcomes?What are the particular
mechanisms by which a treatment achieves its successful
outcomes?
As a rule, psychodynamic therapy
appears to be based on the theory that mental illness is
rooted in unconscious conflicts -- not necessarily conflicts
over sex and aggression like the Oedipus conflict, but
unconscious conflicts nonetheless; and that uncovering these
conflicts is the key to successful therapy. However, there is
very little scientific evidence that unconscious conflict lies
at the root of major forms of mental illness, such as
schizophrenia, anxiety disorder, or depressive disorder. And
there is no scientific evidence that the primary goal of
psychodynamic psychotherapy, which is to bring such conflicts
into the daylight of consciousness, is the key to successful
treatment. Rather, the evidence seems to indicate that the
success of psychodynamic psychotherapy, where it achieves such
successes, is produced by the same sorts of techniques
employed by cognitive-behavioral psychotherapists -- namely, a
focus on the here and now, as opposed to the there and then.
There is also the matter of utility. If
psychodynamic psychotherapy achieves its positive outcomes by
the same mechanisms as cognitive-behavioral therapy, but takes
longer and costs more, then cognitive-behavioral therapy is to
be preferred on grounds of cost-effectiveness. CBT is not just
based on more scientifically valid conceptualizations of
mental illness -- it also delivers more bang for the buck.
Here's an example of the kind of
comparison I have in mind: a study of treatment for eating
disorder (specifically, bulimia, with its characteristic cycle
of binge eating and purging), which compared
psychoanalytic psychotherapy and cognitive-behavioral therapy
(Poulsen et al., Am. J. Psychiat, 2014).
Patients were randomly assigned to one treatment or the
other. The psychoanalytic treatment encouraged patients
to talk about threatening, repressed, feelings and desires,
and how they might be related to eating disorder. The
CBT treatment challenged the patients' beliefs that their
self-esteem was determined by their body weight and size, and
promoted healthier eating patterns. The psychoanalytic
treatment continued for up to two years of weekly sessions,
while the weekly sessions of CBT lasted only 5 months.
Nevertheless, CBT delivered clearly superior outcomes:
At the end of the 5 months, 42% of patients ceased binging and
purging; treatment; the comparable figure for the
psychoanalytic treatment, after the same amount of time, was
only 6%. After the full two-year treatment, only 15% of
the patients in the psychoanalytic group showed
remission. There was some relapse in the CBT group,
after 19 more months, but even so 44% of patients remained in
remission -- a numerical increase over the outcome at 5
months. There was no untreated control group -- which is
unfortunate, as spontaneous remission has been known to occur
even in the case of eating disorder (Vandereycken, Eating
Disorders, 2012), but even so there was a clear
advantage for CBT over psychoanalysis. Not only was CBT
more effective, it was also more efficient: it took less time,
and it was delivered by therapists who had less formal
training than the psychoanalysts. The study is
remarkable in that the senior authors, Stig Poulsen and
Susanne Lunn, were themselves psychoanalysts, and had devised
the psychoanalytic treatment regime they tested. Their
treatment came out on the short end of the comparison, but
they published it anyway.
On those grounds, it seems that CBT
still has an edge over psychodynamic psychotherapy. But again,
a precise answer to the question will depend on the particular
disorder being treated.
Psychotherapy vs. Medication
How does psychotherapy
stand up, in comparison to medication? This question
has often been investigated in the context of
depression. In a provocative article entitled
"Listening to Prozac But Hearing Placebo", Kirsch
& Sapirstein (Prevention & Treatment,1998) conducted a
meta-analysis of 19 published studies in which an
antidepressant medication (such as Prozac) was
compared to placebo, and another
19 studies comparing psychotherapy with a
wait-list or no-treatment control. Putting
the four conditions together, they
provided a comprehensive
overview of the outcomes of
various treatments for
depression.
The
median effect size (D) for
the drug groups was 1.55 standard deviations (SDs),
while D for the placebo was 1.16 SDs.
The
three types of antidepressant medication used
in these studies did not differ
significantly in effect size: tricyclic and
tetracyclic, D = 1.52; SSRIs, D
= 1.68; Other, D = 1.43.
The mean D for psychotherapy was
1.60, about the same as for drug
treatment (this is a common
finding), compared to D =
0.37 for the controls.
Unfortunately, K&S did not
compare different forms of
psychotherapy.
So, some depressed patients get better on
their own, without any treatment -- a phenomenon called spontaneous
remission. Apparently, over
the natural history of an acute
episode, depression sometimes goes
away all by itself. Active
treatment improves the prospects of a good outcome
considerably, but the outcome with
psychotherapy alone is about the same as the outcome with
drugs alone. And so is the outcome with placebo
medication -- though, frankly, if you think about it,
the placebo group is really another
form of psychotherapy. The patients who received
placebo received all the attention, social support,
and the like that the drug patients received -- only
without the active drug (it's findings
like this that give rise to the Dodo Bird Verdict). On the basis of
their results, K&S concluded that the
active ingredients in antidepressant medications accounted for
about 25% of the outcome in the
drug treatment of depression; spontaneous remission
(natural history) accounted for
another 24%, and placebo accounted for
approximately 51%.
The point of all this
is not to diminish the value of
antidepressants: there's that 24%,
which is not nothing.
Kirsch's data is convincing, but
Kramer's response is probably
correct: when people are depressed,
the combination of drugs and
psychotherapy can be very
helpful. The point is that
even powerful psychoactive drugs
have substantial placebo components, and this is likely to be true
for the major and minor
psychedelics as well. As
Kirsch et al. (2002) point out,
"Placebo alcohol produces
effects that are not observed
when alcohol is administered
surreptitiously...".
If pharmacotherapy is effective, and
psychotherapy is effective, what about the combination of the
two?Here the data is
somewhat in flux, but it appears that the combination of drugs
and psychotherapy is rather promising. In a study by Keller et
al. (2000), depressed patients who received
cognitive-behavioral therapy did about as well as those who
received Serzone (Nefazodone), an SSRI, but those who received
them both did especially well.
Here's another example. Obsessive-compulsive disorder,
like many other anxiety disorders, is commonly treated with
SSRIs -- even though there are perfectly good
cognitive-behavioral therapies for this problem. But
SSRIs aren't always effective, or at least they aren't always
as effective as we'd like them to be. In a randomized
clinical trial, Simpson et al. (JAMA 2013) studied a
group of patients with OCD who did not respond positively to a
course of treatment with SSRIs. One subgroup got an
additional medication, the antipsychotic Risperidone
(remember, "antipsychotic" drugs are really little more than
major tranquilizers); another got a placebo pill; and a third
group got a course of cognitive-behavioral therapy emphasizing
exposure and response prevention (i.e., a variant on
flooding). The outcome was measured with the Yale-Brown
Obsessive-Compulsive Scale, a standardized instrument used in
the diagnosis of OCD. The risperidone didn't help much:
only about 23% of the patients got better 13% were essentially
"cured"), compared to 15% (5% "cured") for placebo. But
the cognitive-behavioral therapy helped a lot: 80% of
the patients in this treatment group got significantly better,
and 43% were essentially "cured". One wonders what would
have happened if these patients had simply gotten the CBT,
without any drugs at all. Or, whether patients who
responded well to the SSRI would have done just as well, or
even better, if they received CBT as well. Or, if those
patients had just gotten CBT, without any drugs at all.
The fact of the matter is that, for
people with mild or moderate cases of depression, anxiety, and
many other mental illnesses, psychotherapy -- especially some
form of cognitive-behavior therapy -- works about as well as
medication. Medication really boosts treatment outcome
only in severely ill patients. For people with mild to
moderate illnesses, psychotherapy alone reduces side effects
(obviously, because patients don't get medication in the first
place) as well as the risk of relapse as the treatment
proceeds and the patient is improving and recurrence of a new
acute episode after full remission.
There is also evidence that
psychotherapy is associated with lower relapse rates than
medication. In a study of depression, patients were
administered either an antidepressant SSRI or
cognitive-behavioral therapy. Patients in both groups
responded equally well to treatment. But when the patients
were followed up some time after their medication was
discontinued, or therapy terminated, the patients in the
medication group were much more likely to have relapsed --
that is, to have experienced another episode of depression. In
other words, psychotherapy came closer than drugs to providing
a cure for depression.
And a meta-analysis by Swift et al. (Psychotherapy,
2017) found that patents who receive psychotherapy are less
likely to drop out of treatment, or to refuse treatment in the
first place. These investigators analyzed studies that
compared psychotherapy and pharmacotherapy, alone and in
combination. It is standard practice in these sorts of
studies to report the number of patients who refused their
assigned treatment, as well as the number who dropped out
before completing it. Patients assigned to
pharmacotherapy alone were more likely to refuse treatment
than those assigned to psychotherapy alone, or to a
combination. Similarly, patients were more likely to
prematurely terminate treatment if assigned to pharmacotherapy
alone. People seeking help for mental and behavioral
problems appear to prefer the personal contact that comes with
psychotherapy; if they're going to get medication, they want
the dialog and social support that comes with a live
therapist, too. So, even if mediation is the primary
vehicle for treatment, supplying adjunctive psychotherapy may
help patients stay on course.
Combining psychotherapy with medication
often seems like the optimal approach to treatment.
Presently available psychiatric drugs offer a fair measure of
symptom relief, but not a cure. Psychotherapy gives the
patient the knowledge and skills to overcome his illness, or
at least to cope with it more effectively. In the Keller
study, patients who got Serzone experienced a temporary boost
in their mood, and that's not a trivial outcome. But patients
who got active psychotherapy learned to deal with their
depression on an ongoing basis, and to adjust to the life
after the depression went away. More generally, patients can
suffer relapses when their drugs are withdrawn, but in a sense
new knowledge and skills, acquired through the experience of
cognitive-behavioral therapy, never go away. They remain
permanently available to the patient, as part of his
repertoire of social intelligence.
It's probably for this reason that
patients who receive psychotherapy, regardless of whether or
not they also receive drugs, are less likely to relapse before
full remission, or to experience a recurrence of another acute
episode. On the other hand, there is some evidence that
medication can actually interfere with psychotherapy
(Forand et al., 2013). For mild to moderate cases,
psychotherapy does about a well as drugs -- with fewer
side-effects and less risk or relapse or remission.
Drugs are most effective for the most severe cases -- and even
then, psychotherapy can help, by giving the patient new
knowledge and skills.
And of course, effective psychotherapy
avoids the unpleasant and harmful side-effects of
medications. A good example is insomnia, a
fairly common sleep disorder, and one of the prominent
symptoms of depression. Patients with insomnia are often
treated with prescription medications such as Ambien and
Lunesta, as well as sedative drugs like the benzodiazepines,
and over-the-counter "sleep aids" such as ZzzQuil. But
all of these drugs carry a risk of dependence, if not
addiction; they can make the patient feel groggy even during
the daytime; they can disrupt the REM (dreaming) stage of
sleep. But an effective psychological treatment,
Cognitive-Behavioral Therapy for Insomnia (CBT-I), achieves
the same success rate as medications, without the side effects
(Morin et al., 1994, 2006).
Interestingly, a course of CBT-I is also effective in
lifting depression, roughly doubling the effectiveness of
conventional treatments. What's interesting about
this is that we usually think of insomnia as a symptom of
depression -- that is, as something that is caused by an
underlying mental illness. But it's also possible that the
relation between depression and sleep is bidirectional --
that is, that insomnia may exacerbate the individual's
depression, and treating the insomnia will also cause the
depression to life, at least a little. At least the
patient won't be depressed about not getting enough sleep!
Or, it may be that conventional treatments don't do
anything for the disordered-sleep component.
Or, it may be that gaining control over sleep may
improve the patient's sense that he can get control over
the other symptoms, as well.
The combination of drugs and
psychotherapy is probably no less important in schizophrenia
than it is for depression. We know that a wide range of
social stressors can be implicated in the onset of
schizophrenia, and it makes sense that eliminating or at least
modulating these aspects of the environment would promote
successful treatment. Equally important, people with
schizophrenia may have to learn how to live with their
disability, and these cognitive and social skills must be
learned through active rehabilitation programs. (See "A
Social Salve for Schizophrenia" by Matthew M. Kurtz, Scientific
American Mind, March-April 2013).
Recent reviews show that these programs can, in fact, be
successful (Horan et al., 2011; Kurtz & Richardson,
2012).
Identifying people at risk for schizophrenia, and
helping them acquire these skills, may even prevent the
occurrence of the illness in the first place.
In the words of the ancient adage (sometimes attributed to Lao
Tze in the Tao Te Ching -- though I can't find it in
my copy):
Give a man a fish and he eats for a
day. Teach a man to fish and he eats for a lifetime.
Giving a patient drugs is like giving a
man a fish: when they're gone they're gone. But the learning
that comes through active cognitive-behavioral psychotherapy
stay forever, as a permanent resource for the patient.
The Social Context of Psychopathology
Traditional
forms of psychotherapy, including psychodynamic and
cognitive-behavioral forms of therapy, tend to treat the
individual patient in isolation -- there's the therapist, and
there's the patient, and that's about it. This tradition
follows from the medical model, in which the patient has some
illness that the doctor treats with an antibiotic, or surgery,
or whatever. But psychologically speaking, we've already
argued that, as the poet John Donne put it "no man is an
island". Psychology explains the individual's behavior in
terms of his or her individual mental states, and that goes as
well for abnormal behavior, as well as for the psychological
deficits and maladaptive social learning that account for it.
Individuals live their lives in the context of other people,
and it would be foolish to assume that the social context has
no influence on individual mental patients and the course of
mental illness.
In fact, we've already seen how certain
anxiety disorders, such as phobias and obsessive-compulsive
disorder, can be acquired through social learning, as well as
through direct experience. And also how expressed emotion --
how other family members view and behavior toward the patient
-- can influence the prospects for recovery and relapse in
patients with schizophrenia.
The role of social factors in
psychopathology can be seen in the various "epidemics" of
mental illness:
Multiple Personality Disorder in the 1980s
Attention deficit Hyperactivity Disorder in the early
21st century.
Group and Family Therapy
Some therapists have gone so far as to
assert that it is not enough to treat the individual patient,
precisely because, in some psychologically real sense, it's
not just the patient who is mentally ill. And if it's not just
the patient who is mentally ill, then it's a mistake to treat
the individual patient as if he or she were the only person
that mattered. If the real problem is with the patient's
relationship with other people, then it's the relationship
that has to be treated. At the very least, other people have
to be enrolled somehow in the treatment process.
This is obviously the case with many
problems in living, such as marital difficulties, that are
often treated by psychotherapists. If a marriage is in
trouble, you can't hope to fix it by working on only one
partner. Both partners have to be in the therapy, together.
Many patients are treated in groups in
addition to, or instead of, individual therapy sessions.
Group therapy has obvious economic advantages, and
psychological advantages as well. Patients can learn
that other people have problems like theirs, and learn how
others deal with them. Individual patients can find
social support and encouragement for their own efforts to get
better, and models for improvement. Some patients'
problems are best observed in a group context. And the
group provides a "safe place" where patients can try out new
ideas, feelings, and behaviors.
Alcoholics Anonymous is an informal
setting , created and maintained by recovering alcoholics
themselves, which provides many of the benefits of group
therapy.
Among
the earliest and most vigorous proponents of this idea was
Salvador Minuchin (Minuchin et al., 1974), a psychiatrist who
has specialized in the treatment of eating disorders in
adolescents. Minuchin argued that mental illness should not be
construed as "contained within the individual"; nor should the
mental patient be viewed as a "passive recipient of noxious
environmental [or biological] influences. Rather, Minuchin
argued that family (and other social) interactions may be
responsible for certain forms of mental illness; and that
these family interactions are truly interactional in
nature, in that the patient plays a role in shaping the
environment to which he or she, in turn, responds.
Minuchin's open
systems model of psychopathology and psychotherapy
"[broadens] the focus from the sick child to the sick child
within the family" and "redefines the nature of pathological
disorder and the scope of therapeutic change" (Minuchin et
al., 1974). The open systems model postulates that:
The way the family is organized is triggers the
development and maintenance of the child's symptoms.
The child's symptoms themselves help maintain that very
same family organization.
Minuchin et al. conclude: "Therefore,
therapy must be directed toward changing the family processes
that trigger and maintain the child's... symptoms and toward
changing the use of these symptoms within the family."
Obviously, that can't be done with the child alone; and it
can't be done by working on one family member at a time. The
whole family has to be enrolled in the treatment of the child,
and the whole family has to change.
Minuchin et al. go on to
describe a pathological family organization in terms of
several family transactional characteristics:
Enmeshment, or a high degree of responsiveness and
involvement with the child, so that any change in one
family member will "reverberate throughout the family
system".
Over-protectiveness, in which family members' concerns
for each others' welfare go far beyond the bounds of any
individual's illness.
Rigidity, such that family members are committed to
maintaining the status quo in the family, to such an
extent that, quite literally, they prevent the child from
getting better -- precisely because any change in the
child would disrupt the family's organization.
Lack of conflict resolution, which prevents families
from acknowledging and negotiating various problems.
Minuchin et al. devised a form of family
therapy that was expressly designed to identify,
challenge, and break down these four characteristics, and thus
create a family environment in which the child is permitted,
and encouraged, to get well. For example, it wasn't just the
individual child who was hospitalized for treatment; the whole
family had to stop what it was doing and mobilize for
treatment. Minuchin's system was further developed by a group
of therapists at the Maudsley Hospital in London (yes, that's
the old "Bedlam", now much reformed and one of the world's
leading centers for research on psychopathology and
psychotherapy), and is now known as the "Maudsley model" for
family treatment of adolescent eating disorders.
In their initial 1974
study, Minuchin et al. reported about 86% success in treating
48 children with "superlabile" diabetes, "intractable" asthma,
or anorexia nervosa, but they did not have a comparable group
that received traditional individual therapy. The comparison
of family vs. individual therapy has been carried out mostly
by the Maudsley group, who largely confirmed Minuchin's
findings.
For example, Russell et al. (1987) reported that, after
1 year of treatment, family-based treatment (FBT) for
eating disorder (both anorexia and bulimia) produced
significantly better outcomes than individual treatment
(IT), especially for patients whose illness had began in
childhood or adolescence.
Interestingly, a 5-year followup of these patients by
Eisler et al. (1997) found no difference between the two
groups, indicating that the patients who had received
individual treatment eventually got better as well. But
that doesn't mean that the FBT and were equally effective.
Most patients with eating disorder will, eventually, "grow
out" of their disorder in the natural course of time. But
in the meantime their lives, and their families' lives,
are hell, and there are significant risks to the patients'
health while the illness runs its course. So anything that
gives the natural course of the illness a boost is a good
thing -- and FBT is a much better booster than IT.
Chronic Disease Management and Rehabilitation
What about instances of
mental illness where a cure is impossible? There are lots of
such disorders, including:
the organic brain syndromes (brain damage is, for all
intents and purposes, irreversible);
intellectual disability (most syndromes can't be
reversed or prevented);
schizophrenia (the tranquilizers are tranquilizers, not
cures);
autism (no cure yet, though some behavioral treatments
can effectively convey important social skills);
relapsing mood or anxiety disorders (relapse is likely
when the drugs are discontinued).
After the acute phase of mental
illness, after efforts at treatment have gone as far as they
can, the patient may move into a chronic phase. Such
circumstances call for rehabilitation programs to help
patients and others cope with their chronic disability, get
out of the institution, back to their families and
communities, and make an optimal social adjustment despite
their illness.
Mental Hospitals
Before the 19th century, there was
little by way of active treatment or rehabilitation.
Psychology wasn't yet a science, nor was psychiatry a branch
of medicine -- and never mind that medicine wasn't all that
scientific, either!
For the most
part, mental patients, when they became too much trouble, were
simply warehoused -- often, kept in prisons along with
criminals. Sometimes, they were housed in special "insane
asylums", separate from convicts. A good example of an
18th-century insane asylum is the Royal Bethlehem Hospital in
London, founded in 1337 as a religious charity, then taken
under royal auspices in the 16th century. But even these
hospitals could offer little more than custodial care, and
conditions in most of them progressively deteriorated. Which
is how the Royal Bethlehem Hospital got the nickname "Bedlam".
In fact, the middle and upper classes used to pay a fee to
visit the hospital and watch the antics of the patients as a
form of Sunday-afternoon entertainment.
"Bedlam" and The Rake's Progress
The word bedlam has
come to mean "a state of uproar or confusion", but the word
has its origins as the popular name of the Royal Hospital of
St. Mary of Bethlehem, in London. Bedlam, originally founded
as a charity hospital in the 14th century, had by the 18th
century become a notorious madhouse, and was depicted in
William Hogarth's A Rake's Progress, a series of
eight paintings (also published as engravings, with the
images reversed) produced in 1733-1735. In the sequence, Tom
inherits a fortune from his father, abandons his finance,
Sarah Young, who is pregnant with his child, and moves to
London to live the high life. He leads a life of increasing
dissolution, falls into debt, and marries a rich but ugly
spinster, but he gambles away her fortune as well. He is
incarcerated in debtors' prison, but goes mad (perhaps
suffering from dementia caused by syphilis) and is consigned
to Bedlam.
The Bedlam scene has been described as an
authentic representation of the interior of the hospital as
it existed in the 18th century -- with individual cells,
men's and women's quarters separated by an iron grate,
hospital staff, potentially suicidal patients (like Tom)
chained to the walls, sightseers who paid a tuppence to view
the patients' antics, and Sarah kneeling beside Tom.
See "A Rake's Progress: 'Bedlam'" by James C.
Harris,Archives of General Psychiatry, 2003).
Hogarth's series of engravings was the inspiration for The
Rake's Progress, an opera by Igor Stravinsky, with
libretto by W.H. Auden and Chester Kallman (1951).
Even though Esquirol distinguished
between the mentally ill (in his terms, the insane), the
intellectually disabled (in his terms, the mentally
deficient), and mere criminals, they were still all housed
together (except for insane members of upper-class families,
who were more likely to be consigned to the attic, as in
Charlotte Bronte's Jane Eyre). Things began to change
when Philippe Pinel (1745-1826), became the superintendent of
the Bicetre, an asylum in Paris, and later the Salpetriere, a
large mental hospital (which you can still see when you visit
the city). Along with his mentor, Jean-Baptiste Pussin
(1745-1811), Pinel pioneered the "moral" treatment of those
who, although mentally ill, still deserved respect as
"citizens". Pinel is also credited with freeing the mentally
ill from their chains -- although it was actually Pussin who
did this (and he replaced the chains with straitjackets!).
The
moral, humane treatment of the mentally ill quickly spread to
England and America. Bethlem Hospital was reformed. In 1792,
Benjamin Rush (1745-1813), a physician who had been one of the
signers of the Declaration of Independence, founded a division
of the Pennsylvania Hospital (itself the first hospital in
America, after New York's Bellevue), devoted to the moral
treatment of the insane. Rush's treatise, Medical
Inquires and Observations Upon diseases of the Mind
(1812) was the first textbook of psychiatry published in
America. Another book, On the Construction,
Organization, and General Arrangements of Hospitals for the
Insane (1854), by Thomas Kirkbride, the first
superintendent and physician-in-chief of the Institute,
remained influential even into the 20th century. (I worked at
The Institute as a graduate student at the University of
Pennsylvania).
For more on Benjamin Rush, see "Rush's
Remedies" by Susan Frith, Pennsylvania Gazette,
07-08/2012, and "A New Founding Mother" a sketch of Rush's
wife, Julia, by Stephen Fried, Smithsonian,
2018.. Also Fried's biography of Rush, Rush:
Revolution, Madness, and the Visionary Doctor Who Became a
Founding Father(2018).
There was also an extensive system of
private mental hospitals, catering mostly to the wealthy. An
early example was the Sidis Institute at Maplewood Farms, a
large estate in Portsmouth, New Hampshire. Established by
Boris Sidis, a friend of William James, and leader of the
"Boston School" of psychotherapy (and father to William James
Sidis, at the time the youngest person ever to enter Harvard
College, at age 11), the Institute offered all the latest
treatments, including psychotherapy in an environment of
"beautiful grounds, private parks, rare trees, greenhouses,
sun parlors, palatial rooms, luxuriously furnished private
baths, private farm products". By 1916, there were more than
20 such institutions in Massachusetts alone.Link to the
Sidis Institute website.
Still, some of these asylums were awful
places, little better than bedlam. In 1845, the British
government set up the independent Lunacy commission to set and
enforce standards for private mental hospitals. For a
history of mental-hospital reform in Victorian England, see Inconvenient
People by Sarah Wise (2013).
By
the late 19th century publicly supported mental hospitals were
a feature of virtually every state health system. These were
often glorious structures, architecturally distinctive
-- following the precepts laid down by Thomas Kirkbride (see Asylum:
Inside the Closed World of State Mental Hospitals by
Christopher Payne (2010).
Binghamton State Hospital, near where I grew up in New
York State, was a neo-Gothic structure, built in 1858, and
situated on a hill overlooking the city like some medieval
castle. It's on the National Register of Historic Places.
Napa State Hospital, erected in Northern California in
1872, also a neo-Gothic structure, included farming
operations designed to make the hospital self-sufficient,
and also to provide a kind of occupational therapy for the
residents.
Oregon State Hospital, in Salem, was the setting for Ken
Keesey's novel, One Flew Over the Cuckoo's Nest --
location for the film made from the book. Its
classic building has now been re-purposed as a Museum of
Mental health, which tells the story of public,
state-funded mental hospitals.
Here are some more classic state mental
hospitals.
The Trans-Allegheny Lunatic Asylum,
built between 1858 and 1881, in Weston, West
Virginia. Now closed, it still hosts guided
tours. See "Getting Into the Spirit" by John
Searles, New York Times 10/13/2013.
The South Carolina State Mental
Hospital, in Columbia, was designed in Italian
Renaissance Revival style by the same architectwho
designed the SC State Capitol. Built beginning
in 1857, it replaced the earlier South Carolina
Lunatic Asylum (1828), which was the first public
mental hospital in the South, and only the third in
the nation. Decomissioned in 1990, it remained
an important feature in downtown Columbia, and was
slated to be converted into luxury apartments before
it was destroyed by fire in September 2020.
Greystone Park Mental Hospital, in New
Jersey. Like the Trans-Allegheny Asylum, Greystone was
designed as a "Kirkbride
building", following the principles of "moral
treatment" of the insane promoted by Thomas Story
Kirkbride, who trained, and later ran, the Institute
of the Pennsylvania Hospital in Philadelphia.
Woody Guthrie, the American folksinger, was a patient
here from 1956 to 1961 (when Guthrie told the staff
that he had written 8,000 songs, he was diagnosed as
having "grandiose ideas" and as lacking in "judgment"
and "insight". As of 2015, Greystone Park was
slated to be demolished, although a group of
preservationists were trying to save it as an
important historical landmark. See
"Preservationists Fight to Save a Former Mental Asylum
in New Jersey" by Dan Hurley, New York Times,
04/03/2015).
But as good and humane as these
hospitals were intended to be, they still offered little more
than custodial care until the beginning of the 20th century,
when advances in psychology and psychiatry began to afford the
possibility of active treatment of the mentally ill. In the
20th century, reflecting our progressively increased
understanding of mental illness, public and private mental
hospitals offered active treatments as well as custodial care:
biological treatments like psychosurgery, ECT, and later drug
treatments of various kinds, as well as psychotherapy by
psychologists and social services by social workers.
A 1946 expose by Life magazine
described many American asylums as "little more than
concentration camps".
All that came to a screeching halt with
the de-institutionalization movement that began in the
1960s, when the mental hospitals began to be emptied and their
residents discharged back to their families and communities.
Partly this was a result of the early successes of the
pharmaceutical revolution, which made many schizophrenics more
manageable, and afforded symptom relief to many with patients
suffering from depression and anxiety disorder. In addition,
most public mental hospitals suffered from overcrowding, and
budget difficulties led to a lack of properly trained and
supervised staff, and corresponding scandals of the sort
exposed by Life magazine. But there were also
other contributing factors:
There arose an anti-psychiatry movement which
questioned not only the existence of mental hospitals, but
the whole idea of the mental-health professions.
Thomas Szasz (1920-), influenced by a radically
libertarian political philosophy, argued in his book,The
Myth of Mental Illness (1960) that, aside from
actual neurological disorders, most of what we call
"mental illnesses" were simply "problems in living" and
psychiatry ought to mind its own business.
Theodore Sarbin (1911-2005), a social psychologist
(who taught at Berkeley before moving to the then-new UC
campus at Santa Cruz), also argued that mental illness
was a myth, born of a mistaken metaphor with physical
illness. For Sarbin, mental illnesses was a role imposed
on individuals whose behavior deviated from prevailing
social norms.
R.D. Liang (1927-1989), influenced by the 60's passion
for psychedelic drugs, argued that, far from being
symptoms of some kind of medical disorder, what we call
"mental illness" was really an episode of transformation
not unlike what Native Americans experience in their
"vision quests".
Any way these and other
writers looked at it, then, the mentally ill didn't belong
confined in mental hospitals -- or even treated as if they
were really ill.
The burgeoning civil rights movement of the 1950s and
1960s expanded into a movement for the rights of disabled
people -- including the mentally disabled. Under a
doctrine of "least restrictive conditions", the law came
to the view that disabled people had a right to live with
the least restrictions possible. For people in
wheelchairs, that meant that public accommodations had to
build ramps, and widen their doorways. For people with
mental illnesses, that meant no more confinement in mental
institutions.
In 1967, the New York Civil Liberties Union
established its project on Civil Liberties and Mental
Illness.
In 1971, Frank Johnson, a federal district court judge
in Alabama, decided (in Wyatt v. Stickney) that
patients in a state mental hospital had a constitutional
right to treatment, not mere confinement.
In 1972, a similar case in New York, concerning the
residents of the Willowbrook State School for what was
then called the "mentally retarded" (New York ARC v.
Rockefeller), required the state to facilitate
community placement of intellectually disabled
individuals
In 1973, the American Civil Liberties Union followed
suit, with its Mental health Law Project.
In 1975, the United States Supreme Court unanimously
decided (in O'Connor v. Donaldson, also argued
by Ennis) that patients involuntarily confined to mental
hospitals were constitutionally entitled to effective
treatment. Agreeing with a lower court decision,
the Court declared : "a State cannot constitutionally
confine... a non-dangerous individual who is capable of
surviving safely in freedom by himself or with the help
of willing and responsible family members or
friends...".
In 1990, the Americans with Disabilities Act (ADA)
required that individuals with physical and mental
disabilities be allowed to live in the least restrictive
setting possible; and, wherever possible, to be
integrated with non-disabled individuals.
In 1999, the requirement that mentally ill people be
able to live in the least restrictive settings possible
was affirmed by the United States Supreme Court in Olmstead
vs. L.C.
In 2010, the Affordable Care Act (ACA, aka Obamacare)
listed mental health and substance abuse services among
10 "essential health benefits", and mandated parity
between physical and mental illnesses. The ACA
also included federal subsidies permitting individuals
under 65 years of age to receive community mental health
services (individuals over 65 were already covered in
this respect under Medicare), and expanded mental-health
coverage for the poor under Medicaid.
Anne Harrington, in The Mind Fixers (2019;
described earlier) argues convincingly that
de-institutionalization, while aided by the availability
of various psychiatric drugs, was also promoted by
Freudian psychoanalysts and other psychotherapists .
And then, of course, there was the economy.
Hospitalization is expensive, and as states looked for
ways to tighten their budgets, public mental hospitals
were an easy target.
The federal government encouraged
de-institutionalization as well, for both economic and legal
reasons. But the funds promised to support community and
family treatment of de-institutionalized mental patients never
were forthcoming -- with the result that homeless people with
mental illness and substance abuse are found on the streets of
every major city (if you don't believe me, check out Peoples'
Park in Berkeley, or Civic Plaza in San Francisco).
For excellent journalistic coverage of the
de-institutionalization movement, see:
No One Cares About Crazy People: My Family and the
Heartbreak of Mental Illness in America by Ron
Powers (2018), both of whose sons suffered from
schizophrenia -- and who, he argues, would have received
better treatment in a mental hospital than in the
community.
Insane: America's Criminal Treatment of Mental
Illness by Alisa Roth (2018), who argues that jails
and prisons have become dumping grounds for the mentally
ill, who receive little or no treatment for their
illnesses while they are incarcerated.
De-institutionalization was not a bad
idea. There were, admittedly, lots of people confined to
mental hospitals who didn't need to be there. At the same
time, it's not at all clear that the homeless mentally ill are
better off on the streets of Berkeley and San Francisco than
they would be within the walls of Binghamton or Napa State
Hospital. Moreover, mental hospitals could have created an
environment for the active rehabilitation of the mentally ill,
preparing them for lives in the community and with their
families. Such environments are going to look
increasingly attractive as an aging population of Baby Boomers
increases the number of individuals with Alzheimer's Disease
and other forms of dementia, and individuals on the autism
spectrum outlive their parents and other family members who
have cared for them.
And community mental health treatment
isn't always all it's cracked up to be, either. All too
often, substandard care in large state institutions has been
replaced by substandard care, barely better than custodial
care, in small group homes, run on tight budgets, by
individuals who, however well-intentioned they may be, often
lack proper training and supervision. And then again,
many of these group homes are run on a for-profit basis,
further limiting the care and support that the
non-institutionalized mentally ill receive. Many
homeless mentally ill and up in local jails, for want of any
other way of housing them -- a step backward, I suppose,
toward the moral model of mental illness.
For this reason, some prominent
psychiatrists have begun to advocate for a revival of the
state mental hospital system for the care of the chronically
mentally ill (see "Improving Long-Term Psychiatric Care: Bring
Back the Asylum" by D.A. Sisti, A.G. Segal, and E.J. Emanuel,
Journal of the American Medical Association,
2015). The same legitimate concerns that led to
de-institutionalization in the first place will probably
oppose any such move (see, for example, "Under Lock & Key:
How Long?" by Aryeh Neier & David J. Rothman, New York
Review of Books, 12/17/2015). But if re-institutionalization
occurs, we can hope that it avoids the problems that cropped
up in the 20th century. That will take money, for proper
facilities and proper staffing; and strict enforcement of the
legal principle of "least restrictive treatment". The
mental hospital may have its place in public policy, but
nobody should be sent there who can't receive safe, effective
treatment in the community.
For better and for worse,
de-institutionalization is a fact of life in the United
States, and many other developed countries as well. But
in underdeveloped countries, institutionalization remains the
norm, and the institutions themselves are often little more
than warehouses for the mentally ill. In 2013, the World
health Organization introduced a "global mental health plan"
to move from centralized mental hospitals to community-based
care. But this takes money -- money that is hard to come
by even in a rich country like the United States, and even
harder to come by for the underdeveloped countries of the
Third World. (For more information, with a special focus
on developments in Guatemala, see "Where Mental Asylums Live
On" by John Rudolf, New York Times, 11/05/2013.)
Token Economies
Even in the case of the organic brain
syndromes, developmental disorders, and functional psychoses,
behavioral treatments such as token economies,
employing the principles of instrumental or operant
conditioning, can facilitate the acquisition of new, more
adaptive behaviors in individuals with actual or presumed
brain pathology. In token economies, patients receive tokens,
such as poker chips, contingent on their performance of
certain actions, such as cleaning their living area or
dressing themselves; these tokens may then be exchanged for
goods at the hospital canteen or other privileges. In the
language of instrumental conditioning, then, the tokens are
secondary reinforcers. Perhaps as much as medication, these
training procedures help chronic mental patients return to
their families, and live in the community, by providing them
with the repertoire of behaviors they need to live outside the
confines of the mental hospital. (Token economies can also
serve as laboratory models of national economies, but for some
reason behavioral economists haven't taken much interest in
them.)
Social Interventions for Autism
Autism is one of the most challenging
chronic mental illnesses. Psychotropic medication can
help manage some of the secondary symptoms of autism, such as
the mood swings, temper tantrums, and irritability that
autistic children display, but have essentially no impact on
the child's primary deficits in communication and other
aspects of social interaction. For that, the best hope
lies in psychosocial interventions (though injections of
oxytocin have been recommended!).
One intervention technique, derived from
instrumental conditioning, is applied behavior analysis
(ABA), first devised by O. Ivar Lovaas for the treatment of
children with autism. This treatment program involves an
intensive regime, perhaps 40 hours a week (i.e., a full-time
job for both the child and his therapists), beginning very
early (as young as 3 years of age). ABA involves an extensive
system of rewards and punishments intended to shape and
reinforce desirable behaviors, such as making eye contact and
sitting quietly, and to eliminate or discourage undesirable
ones, like yelling or head-banging. Early applications of ABA
sometimes used punishments such as slapping or even electrical
shocks (delivered by an instrument that looked disconcertingly
like a cattle prod), resulting in considerable criticism. Yet
Lovaas contended that his methods delivered results when other
strategies did not, and he eventually gave up punishment in
favor of a regime based entirely on positive reinforcement (in
this respect, following Skinner's dictum that positive
reinforcement is much better than punishment for controlling
behavior). In 1987, Lovaas reported that his treatment had a
50% success rate (a 1993 follow-up showed that most of the
patients had maintained their treatment gains). Subsequent
studies have not reported about a 30% success rate, which is
still better than most other treatments for autism. ABA is
phenomenally expensive, unless you consider the alternatives,
and it is now a standard treatment for autism.
A number of other interventions have
combined techniques from ABA with more cognitive approaches
derived from the study of social development and the "theory
of mind". For example, the Early Start Denver Model
(ESDM) focuses on getting the child to pay attention (and
respond appropriately) to social cues such as facial
expressions, gestures, and -- last but not least -- speech.
Studies have shown that ASDM is effective, but it isn't easy,
one study employing more 2000 hours of therapy delivered over
the course of two years.
Some variant of ABA is the most popular,
and effective, approach to treatment currently available for
autism spectrum disorders (ASD). There is no medication
available, other than sedatives. And although we
generally think of autism as a "chronic" mental illness, from
which a patient will never fully recover, in fact the
prospects for improvement are not trivial. As with
schizophrenia, it is possible for an autistic individual to
make a substantial-enough recovery that he or she will no
longer qualify for ASD.
Fein and her colleagues (2013) identified a group of 34
individuals who had been diagnosed with autism in
childhood but who, as adolescents or young adults, no
longer qualified for the diagnosis. Not all of these
individuals had received ABA, or any formal behavioral
treatment, but most of them, when they did carry the
diagnosis, had milder social symptoms than a comparison
group with "high-functioning" autism.
Lord and her colleagues (2014) followed a group of
patients who had been diagnosed with autism at age 2
(about as early as the diagnosis can be made). By
age 22, about 10% of this group no longer qualified for
the diagnosis. Interestingly, this subset had higher
IQs than those who did not make an "optimal" recovery.
One conclusion from these studies is
that, as with schizophrenia, prognosis is related to premorbid
personality as well as to active treatment. Those
patients who do better, achieving an optimal outcome of their
illness, may be those who have better resources at the start:
better social skills, higher intelligence, and the like.
Cognitive Restructuring -- Again
As discussed earlier, a number of
theorists have proposed that paranoid delusions reflect
schizophrenic patients' inappropriate attempts to explain the
anomalous experiences they have as a result of their illness.
Accordingly, another aspect of rehabilitation may be to give
delusional patients more appropriate and adaptive explanations
for what is happening to them.
When I visited China in 1985, as part of a
delegation of mental health specialists, the mental-health
authorities we meat stressed that the incidence of
schizophrenia in the People's Republic of China was no
different than that in other countries -- which is what we
would expect if schizophrenia was due largely to genetic and
biochemical factors. However, we were also informed that the
incidence of paranoid schizophrenia was lower in China than
in other countries. I have no independent knowledge of
whether this is so, but the attributional account of
delusions offers an explanation for this fact (assuming it
is true): in China, social organization is such that the
mentally ill are detected very early in the acute phase of
their illness, and are brought to local mental hospitals for
treatment. At least at the time of my visit, it was routine
for these acute patients to be given antipsychotic
medication followed by a series of lectures on the nature of
their illness. Perhaps, when schizophrenics in the acute
stage of their illness are given correct information about
what is happening to them, they have no need or opportunity
to develop delusional explanations for themselves.
Rehabilitation is an important aspect of
mental-health treatment because, at least for the present,
most serious mental illnesses, such as schizophrenia, autism,
and the more serious forms of mood disorder, are chronic
diseases: psychiatric medications provide only symptomatic
relief, and psychotherapy can only go so far. For mental
health, as for the rest of medicine, in the face of incurable
illness we do not simply throw up our hands and walk away from
the patient. Nor, for that matter, do we continue fruitless
attempts to cure the patient's illness. Rather, in chronic
illness the goal of treatment shifts from cure to
rehabilitation -- to help the mentally ill become at least
partly self-sufficient, to live on their own or with their
families, or in halfway houses and other protected living
environments. In mental health, as in the rest of medicine,
permanent hospitalization is the last resort.
Stigma, Stereotypes, and the Self-Fulfilling
Prophecy
Unfortunately, the prospects of
successful treatment of mental illness -- whether success
comes in the form of a cure or rehabilitation -- is hampered
by the social context in which mental illness occurs.
People frequently overemphasize the statistical or
social criteria for mental illness, labeling as "sick"
behavior that is simply unusual, infrequent, or
nonconforming. An extreme example of this tendency is the
use of psychiatric diagnosis as a means of social control
-- as in the former Soviet Union, where political
dissidents where frequently diagnosed as mentally ill, and
incarcerated in mental hospitals, simply on the basis of
their disagreement with government policies.
There is also a tendency to embrace the moral rather
than the medical model of mental illness, so that the
mentally ill are perceived as socially undesirable -- as
bad, immoral, or even evil; and as somehow responsible for
their own problems (or, at least, their failure to
overcome them). As a result, people impose a "criminal"
role on mental patients, instead of the "sick" or
"impaired" role, emphasizing restraint and punishment as
opposed to cure or rehabilitation. A familiar example of
this tendency is the stereotypical association of mental
illness with violence and criminal behavior, as well as
the tendency to NIMBYism (as in Not In My Back
Yard) when it comes to the establishment of halfway houses
and other facilities for the community care of the
mentally ill.
And, finally, there is a tendency to identify people
with their illnesses -- particularly their mental
illnesses, by referring to people as schizophrenics
or depressives, rather than people with
schizophrenia or people with depression.
More subtle, perhaps, is the frequent
occurrence of stereotyping when it comes to the mentally ill,
as well as the dominance of first impressions -- psychiatric
diagnoses, once made, tend to stick so that the person never
sheds the label of "schizophrenic", "manic-depressive", etc.,
or for that matter the sick or impaired role. Generally, there
is a popular refusal to admit the possibility of a good
outcome in mental illness -- a successful treatment, whether
cure or rehabilitation, that would allow the person to leave
the sick role and assume his or her proper role(s) in society.
Erving
Goffman, a sociologist, analyzed what he called the stigma
of mental illness. For Goffman, a stigma is "an
attribute that is deeply discrediting" -- which turns a "whole
person" into a "tainted, discounted one". Many physical
stigmata (that's the plural of stigma) are immediately
apparent. But others, like the stigma of mental illness, are
not readily apparent. The mentally ill only become stigmatized
when their mental illness becomes known to others. Before
their conditions become known, the mentally ill, with their
secret stigma, are discreditable; after their
condition becomes known, the mentally ill are actually
discredited.
Following
Goffman, Jones and his colleagues analyzed the stigma of
mental illness in terms of a number of different dimensions.
Concealability: Some stigmata (that's the plural
of stigma) can be concealed, while others cannot. In an
earlier time, being black was stigmatized, but
light-skinned African-Americans were often able to "pass"
for white, and be accepted by white society. The stigmata
of mental illness are not immediately apparent, allowing
mentally ill people can "pass" for "normal".
The course of the mark refers to the extent to
which the stigma can be concealed over time. It might be
possible for a mentally ill individual to conceal his
condition for a period of time, but the more time he
spends with other people, the more likely it is that he
will inadvertently reveal his stigma.
Disruptiveness has to do with the extent to which
the stigma can impair the individual's social
interactions.
Aesthetics has to do with other people's
reactions to the stigma.
The origins of the stigma may be congenital
(present at birth) or acquired; if the latter, it may have
been acquired accidentally or deliberately, perhaps due to
some misbehavior on the part of the individual.
Peril has to do with the danger, or the apparent
danger, that the stigma poses to other people.
Link
and Pheelan (2001) offered a different perspective on the
components of the stigma of mental illness.
Social selection is the process by which people
identify and label the differences that are important to
them. Most people don't care whether someone has a
physical illness (unless, perhaps, it's contagious). But
Link and Pheelan argue that people are very much concerned
about mental illness. If someone knows that you've been
diagnosed with schizophrenia, that makes a difference to
them in a way that knowing that you've been
diagnosed with asthma does not.
Stereotyping is the process by which the person's
label, as mentally ill, is linked to a whole list of
undesirable characteristics. If you've got heart disease,
it doesn't matter. But if you've got a mental illness, or
so people think, maybe you shouldn't be around children,
or you're the wrong person for a particular job.
Social selection inevitably leads to a separation
between "Us" and "Them", the stereotyping group,
and the group that gets stereotyped.
The distinction between "Us" and "them" inevitably leads
to discrimination against "Them", and Their loss
of status. This is the discrediting that Goffman
talked about. The discrimination can be direct ("the
mentally ill need not apply") or structural (built into
the structure of society, as when mental hospitals are set
apart from other hospitals). If halfway houses for the
mentally ill are located in less-desirable areas of towns
and cities (as they often are), that carries the
implication that the mentally ill are also undesirable.
And when stigmatized individuals incorporate their stigma
into their self-concept, they may begin to view themselves
as undesirable as well.
And then there is the exercise of power: medical
patients are supposed to follow their doctors' orders, but
they can question them, and challenge them, and seek
second opinions, and do what they want. Mental patients,
because they are presumed to be incompetent mentally,
don't have this same kind of countervailing power.
Considerations
of stigma and stereotyping lead us back to our earlier
discussion of the various construals of deviance.
Applying the statistical and social standards for
abnormality, we can label unusual or nonconforming
behavior as "sick", leading to an inappropriate diagnosis
of mental illness. In the former Soviet Union, people who
were opposed to communism were often diagnosed as mentally
ill and confined to mental hospitals. This still happens
in the People's Republic of China, even today.
Applying the moral vs. the medical model, it is easy to
view the mentally ill not just as socially undesirable,
but also as responsible for their own afflictions. It is
this emphasis on the "criminal role" that led, in the 18th
century, to the confinement of the mentally ill with
paupers and criminals in asylums like Bedlam.
Also subtly keeping the
mentally ill "sick" is the self-fulfilling prophecy
(discussed in the lecture supplements on Personality and
Social Interaction):
the diagnosis of mental illness creates expectations
concerning the patient;
these expectations lead to behavior on the part of
others that elicits abnormal rather than normal behavior
from the patient;
they also lead the patient's normal or ambiguous
behavior to be interpreted by others as "abnormal";
in either case, the patient's behavior is taken as
confirming the diagnosis of mental illness.
Such a process can lead patients to
define themselves as incurably ill, diminishing their
motivation for therapeutic change. It can also lead those who
care for mental patients to substitute custodial care and
medication for active treatment that might return patients to
their normal role(s) in society. If there are few or no
attempts at cure or rehabilitation, we can virtually guarantee
that mental patients will never get well.
A good example comes from schizophrenia,
which is generally thought to have a poor prognosis. In
fact, people with schizophrenia can show a remarkably good
recovery, with treatment, so long as they get the right
treatment, in the right environment -- and, perhaps,
have a "better" premorbid personality to begin with.
Yet another approach to the stigma of
mental illness is simply to deny it. Some individuals
with autism, for example, deny that autism is a mental illness
which should be treated an eliminated. Instead, they
argue that autism exemplifies neurodiversity. In
this view, autistic individuals are not mentally ill -- they
just have brains that operate differently than most other
people. And while they may need help and accommodation
in some respects, they assert that autism isn't something to
be eliminated. Rather, they incorporate autism into
their personal identities.
Temple Grandin is a case in point. Diagnosed with
autism as a child, she grew up to get a PhD and have a
substantial career as a specialist in animal behavior, on
the faculty at Colorado State University. She argues
that her autism gives her a special ability to understand
the interior lives of livestock and other domestic
animals.
I referred earlier to Patricia Harrington's history of
biological psychiatry, The Mind Fixers: Psychiatry's
Troubled Search for the Biology of Mental Illness.
Helen Thomson, reviewing Harrington's book in the New York
Times ("From Schizophrenia to Megalomania, Three New
Books on Mental Illness", 07/07/2019) cites an anecdote about
Shekhar Saxena, director of the mental health unit of the
World Health Organization:
[A]sked where he'd prefer to be if he were
diagnosed with schizophrenia, he said a city in Ethiopia or
Sri Lanka, rather than New York or London. In the
developing world, he explained, he had the potential to find
a niche for himself as a productive, if eccentric, member of
a community, whereas in the modern, Western cities he was
far more apt to end up stigmatized and on the margins of
society.
The "Pseudopatient" Study
The deleterious effects of the social
context on the treatment of the mentally ill are illustrated
by a controversial study reported by David Rosenhan, a
professor of psychology and law at Stanford University, in
1973. In this study, Rosenhan, as well as some colleagues and
students, sought and gained admission to a number of different
mental hospitals, public and private, by falsely reporting
some symptoms commonly associated with mental illness. All the
"pseudopatients" were in their mid-30s (except perhaps for
Rosenhan himself), gainfully employed, with no prior history
of psychopathology, and during the admission interview all the
patients told the truth about themselves except for two
matters:
they did not reveal that they were academic researchers,
or that they worked in an academic organization;
they claimed to be experiencing auditory hallucinations
in which voices spoke such words as "empty", "hollow", and
"thud" (a voice said thud? -- never mind).
Given that hallucinations are serious
symptoms, it is not surprising that all of the pseudopatients
were admitted to the hospital for observation. What is
surprising is what happened next.
Immediately upon their
admission, the pseudopatients ceased their simulation, and
behaved normally in every way (except for identifying
themselves explicitly as simulators). Other patients on the
ward frequently noticed the change, but by and large the
professional staff did not. In fact, Rosenhan reports that the
pseudopatients were largely ignored by the staff.
Most were given a diagnosis of schizophrenia, and their
behavior was interpreted in terms of the diagnosis. For
example, all the pseudopatients kept journals of their
experiences. In the chart of one pseudopatient, this was
described as "patient engages in writing behavior" --
although if the staff had bothered to read what the
patient was writing, his deception would have been
uncovered immediately.
The pseudopatients were given mostly custodial care,
including medications of various sorts averaging 14
capsules per day (they tongued" these pills, and then
disposed of them when they could do so unobserved).
The pseudopatients stayed in the hospital an average of
19 days, at which time most were discharged with the
diagnosis of "schizophrenia in remission" -- notice how
the diagnostic label stuck?
A possibly apocryphal story: In one
particular episode, Rosenhan spent a sabbatical quarter as a
pseudopatient. At the end of the term, when Rosenhan was
obliged to return to his teaching duties, he informed the
attending psychiatrist that he was Prof. David Rosenhan of
Stanford University. The response was "Oh,sure you
are!". Rosenhan's wife had to secure a legal write of habeas
corpus to get him discharged.
And another one. In another episode,
one of Rosenhan's colleagues, an international authority on
depression, while masquerading as a pseudopatient, noticed
that a particular patient was being treated for depression
with an inappropriate drug. The colleague, while staying in
his pseudopatient role, approached one of the ward
psychiatrists to discuss the matter -- identifying himself
merely as someone who had read a lot about depression. After
the discussion, the psychiatrist made a notation on the
pseudopatient's chart that he displayed "grandiosity", and
increased his medication!
A cautionary note: In 2019,
Susannah Cahalan published a book, The Great Pretender:
The Undercover Mission that Changed Our Understanding of
Madness, which was a journalistic inquiry into the
pseudopatient study. Cahalan's previous book, Brain
on Fire: My Month of Madness (2016), was an account of
her own psychotic episode, resulting from a neurological
autoimmune disorder -- a form of encephalitis initially
misdiagnosed as a mental illness. Going through
Rosenhan's papers (he died in 2012), Cahalan was
largely unable to track down the other pseudopatients, or
the raw data for the study he published in Science,
and she strongly implied that he may have fabricated his
data.
That Rosenhan and his collaborators
were admitted to mental hospitals is unremarkable. Anyone who
reports auditory hallucinations deserves some further
investigation. But after their admission, the treatment of the
pseudopatients can only be described as gross negligence.
There was little or no investigation of the "presenting
complaints" that brought them to the hospital in the first
place, and the clinical staff failed to notice that their
symptoms had "remitted". There was little or no active attempt
at cure or rehabilitation, or apparently any consideration
that active treatment was possible.
Although the pseudopatient study is
often cited as an example of the negative effects of the
medical model in psychiatry, it would be more accurate to say
that the problems encountered by the pseudopatients occurred precisely
because the clinicians failed to adhere to the medical model.
If the psychiatrists and others had acted in accordance with
the medical model, they would have discovered much sooner that
the patients' symptoms had disappeared; they would have been
more observant of their behavior; and they would not have been
so quick to dispense medication to patients who did not need
it.
Nellie Bly, Nellie Bly...
Rosenhan and
his colleagues were perhaps inspired by Nellie Bly (the
pen-name -- taken from the song by Stephen Foster -- of
Elizabeth Jane Cochrane Spearman, 1864?-1922), a pioneering
("daredevil" woman investigative journalist. Bly began her
career with the Pittsburgh Dispatch, but became
famous on the staff of the New York World, published
by Joseph Pulitzer (he of the prizes). In 1888, she feigned
insanity to gain admission to New York's infamous
Blackwell's Island insane asylum to gather material for an
expose of patient mistreatment that led to a number of
important reforms in the mental-health system. The series
was subsequently published as a book,Ten Days in a Mad
House (1888).
But Blackwell's hadn't always been that
way. Blackwell's Island, later renamed Roosevelt
Island, and it hosted a hospital (and later a tuberculosis
sanitarium), prison, a workhouse for the poor, and an asylum
for the mentally ill, all in separate institutions.
The whole enterprise was established in 1839 following
passage of a state law requiring that "lunatics" be housed
separately from criminals. But the facilities soon
became overcrowded, and its staffing infected with cronyism,
nepotism. Almost inevitably, and in violation of at
least the spirit of the law, prisoners were employed to take
care of the mentally ill. Charles Dickens visited
Blackwell's Island as early as 1842, long before Nellie
Bly's expose, and was appalled by the conditions he observed
there.
For a history of the public "lunatic"asylum
in New York City, see Damnation Island: Poor, Sick,
Mad, and Criminal in 19th-Century New York by Stacy
Horn (2018).
But this was not by any means Bly's only
accomplishment. In 1890, she beat Jules Verne's fictional
record by traveling around the world in less than 80
days (72 days, 6 hours, 11 minutes, and 14 seconds, to be
exact). After retiring from journalism to run her deceased
husband's companies, she introduced a number reforms for the
treatment of industrial workers, including the provision of
"managed" health care. On vacation in Europe when World War
I broke out, Bly returned to journalism as a war
correspondent for the New York Evening Journal. (By
the way, Bly took her pen name from the popular song by
Stephen Foster, not the reverse.)
Following the Rosenhan study, a Dutch
psychiatric hospital actually commissioned a consulting firm
to plant pseudopatients in its own wards, as a check on
staff behavior and other conditions ("The Doctors Were Real,
the Patients Undercover" by Douglas Heingartner, New
York Times, 12/01/2009).
The issue of how we label
people with mental illness has come to the fore
with the "disability rights" movement, and the objection of people who have
various disabilities to be identified with
their disabilities (a similar issue has been raised in racial,
ethnic, and sexual minority communities as well).
One important question is how to refer
to people with various disabilities. Put bluntly,
should we say that "Jack is a schizophrenic or
"Jack is a person who ha schizophrenia"?
Or substitute any
other diagnostic label, including neurotic, depressive,
or autistic.
Dunn and
Andrews (American Psychologist, 2015) have
traced the evolution of models for
conceptualizing disability -- some of
which also apply to other ways of categorizing
ourselves and others. The current
debate offers two main choices:
A
"person-first" approach
-- as in, "Jack is a person with a
disability". In this
social model (Wright, 1991),
disability is
presented "as a neutral
characteristic or attribute, not a
medical problem requiring a cure,
and not a representation of
moral failing" (p. 258) -- or,
it might also be said, as
a chronic condition
requiring rehabilitation.
Instead, disability itself
is seen as a sort
of social construction
-- or, at least, a
matter of social
categorization.
An "identity-first"
approach -- as in,
"Jack is a disabled
person". While
this might seem a step
backward, this minority
model (Olkin
& Peldger,
2003) "portrays
disability as a
neutral, or even
positive, as well as
natural
characteristic of
human attribute"
(p. 259).
Put another way,
disability confers
minority -group
status: it
connotes
disabled people,
with their own
culture, living
"in a world
designed for
nondisabled
people".
So it all depends on
how you think
about minority-group status -- that of other people, if you're the
member of the
majority; or your own, if you're a member of the
minority (any minority).
Mental-Health Policy
Until recently, the treatment of the
mentally ill was left pretty much in the hands of physicians,
with minimal regulation. Historically, legislatures and courts
have not intruded on issues of medical treatment -- relying,
implicitly on physicians' Hippocratic Oath to "do no harm" --
and also out of respect for the sapiential authority of
physicians, who are assumed to have more expertise in matters
of diagnosis and treatment than laypeople do.
This situation changed sharply in 1971,
in Wyatt v. Stickney, a landmark class-action
case brought against the Alabama state mental hospitals in
1971. Ricky Wyatt (1954-2011) had a record of youthful
misbehavior, as a result of which his juvenile probation
officer arranged to have him committed to Bryce State Hospital
at the age of 14 -- the youngest patient there (the procedures
for such institutional commitment were pretty lax at the
time). Despite the fact that he never actually received a
psychiatric diagnosis, Wyatt was "treated" with large doses of
Thorazine and other antipsychotic medications, and suffered
many other indignities. The Federal judge in the case, Frank
Johnson, ruled in favor of the plaintiffs and placed the
entire state hospital system under federal receivership (where
it stayed until 2003). He also issued a set of guidelines for
the proper treatment of mental patients, now known as the
"Wyatt Standards", that are now applied nationwide. Chief
among these is the concept of least restrictive treatment
-- that if mentally ill or intellectually disabled persons
must be institutionalized, they have a right to as much
freedom as practicable. They also have a right to human
treatment, sufficient staffing, and individualized treatment
plans, plus certain minimal standards for diet and nutrition.
It is no accident that the same judge who ruled in Wyatt
had also earlier placed Alabama's schools and prisons under
federal receivership. The case is a landmark of civil rights
law, and the Wyatt Standards are sometimes known as the Mental
Patients' Bill of Rights.
Another major change in mental-health
policy occurred in 1999, with the White House Conference on
Mental Health and the issuance of the Surgeon General's
Report on Mental Health. The Surgeon General argued that
"mental health is fundamental to health" -- that a sound mind
is part and parcel of a sound body. It also stressed that
"mental health disorders are real health conditions", not
figments of someone's imagination or excuses for not working.
It asserted that "the efficacy of mental health treatments is
well documented" -- a real change from the Eysenck study of
the 1950s, and the Woody Allen Bugaboo. And it noted that "a
range of treatments exists for most mental disorders",
including both biological treatments (like drugs) and
psychotherapy. This was the first time that federal policy
formally recognized the problem of mental illness.
Mental Health Parity
Before this time, mental illness was
treated quite differently from physical illness. While many
consumers has insurance policies like Blue Cross and Blue
Shield to help pay medical bills, they had to pay for
psychotherapy out of their own pockets. And even "Cadillac"
health-insurance plans imposed annual or lifetime dollar
limits on expenditures for treatment for mental illness and
substance abuse. For example, my own health policy at the
University of California, pays for only 28 days of inpatient
mental-health treatment, and outpatient psychotherapy had to
be authorized in a way that outpatient medical treatment did
not.
Now, however, by federal
law, such as the Mental Health Parity Act of 1996,
there is parity between "medical" and "mental" illness.
Health insurance must cover mental health.
Mental health benefits must be subject to the same
annual and lifetime dollar limits as medical and surgical
benefits.
There must be the same schedule of deductibles and
co-payments.
And coverage cannot exempt treatments for behavioral
disorders such as alcoholism, substance abuse, and
chemical dependency.
Still, there remained important gaps
between mental health and other medical services. In
particular, the MHPA control issues like cost-sharing, limits
on number of therapy visits or days of inpatient
hospitalization, and the like. As a result, employers
and insurance companies were able to circumvent the intention
of the Act by increasing patient co-pays for mental-health
services, and imposing limits on the number of visits or the
days of coverage.
The Mental Health Parity and Addiction
Equity Act of 2008 was intended to strengthen parity even
further, by closing the loopholes in the MHPA. It
required that all financial requirements, including
co-payments and caps on visits or days of treatment be the
same for mental-health services as for medical and surgical
services.
So did the Affordable Care Act of 2010 (aka ObamaCare)
reinforced parity -- in fact, one Administration official was
quoted as saying that it was "kind of the final word on
parity" ("Rules to Require Equal Coverage for Mental Ills" by
Jackie Calmes and Robert Pear, New York Times,
11/08/2013).
Its final rules, issued in 2013, concerning "essential
health benefits" mandated that all insurance policies
cover mental-health and substance-abuse treatments.
Co-payments, deductibles, and other limits may not be
"more restrictive" or "less generous" than those that
apply to medical and surgical treatments.
Geographical and facility limitations were also
equalized. If a California resident is covered for cancer
treatment at the Mayo Clinic, in Minnesota, then a
Minnesotan is covered for substance-abuse treatment at the
Betty Ford center in Palm Springs, California.
Whereas the MHPA applied only to group health plans, the
provisions of the ACA apply to all forms of health
insurance.
The precise menu of coverage and services will differ
from state to state, and also depending on the level of
the individual's plan (bronze, silver, gold, or
platinum). The fact that so much variance is
permitted under the ACA does undercut mental-health parity
to some extent, as states and plans may skimp on
mental-health and substance-abuse services. But at least
some coverage is mandatory.
Again, any requirements and restrictions
(such as pre-authorization for treatment) must be the same for
mental health as for other medical care. Still, talk
(legislation) is cheap: the real issue now is enforcement, in
which other budgetary priorities may conspire with the stigma
associated with mental illness, and skepticism about the value
of mental-health treatments, to prevent mental-health services
from actually achieving parity.
In fact, there are serious challenges to
parity for mental-health and substance-abuse services.
In 2017, President Trump and the Republican-controlled House
and Senate attempted to "repeal and replace" the Affordable
Care Act (ACA, aka "Obamacare"). Every attempt to repeal
and replace failed, but by the smallest of margins -- just one
vote in the Senate would have meant major changes to the
funding of mental-health and substance-abuse treatment.
One reason is that one of the "reforms" proposed by the
Republicans was to allow individual states to waive the
requirement that certain "essential services" be covered by
health-insurance policies. Among those "essential
services" most threatened were pregnancy and maternity care,
and -- you guessed it -- mental-health and substance-abuse
treatment. The rationale offered in all three cases
was that because such services were not likely to be needed
by everyone -- only half the population can become pregnant,
for example! -- then only those in need of such services
should have to pay for insurance to cover them. The
argument is bogus, of course: the whole point of
insurance, of any kind, including auto and homeowner
insurance, is to spread the risk, and the costs, among
people who may not need it -- those who may never have an
auto accident, for example, or whose homes might not burn
down. But it's telling that (almost) the first thing
the Republicans promoting health-care "reform" thought of
was to eliminate was parity for mental-health and
substance-abuse services.
Another reason is that each of the Republican proposals
loosened the requirement, under the ACA, that individuals
with pre-existing conditions not be charged more for health
insurance than those without. Individuals already
diagnosed with heart-disease or cancer could not be denied
insurance, under these "reform" plans; but they could be
charged more to be insured against the costs of
treatment. The problem this raises, with respect to
mental-health coverage, is that many mental illnesses, such
as depression, are subject to relapse and recurrence.
If you've already had an episode of depression, even if
you've fully recovered, that may count as a "pre-existing
condition" that will increase your insurance rates.
Moreover, remember that in the diathesis-stress model of
mental illness, some individuals may demonstrate a
relatively poor "pre-morbid adjustment" even before their
first episode. That, too, may be counted as a
pre-existing condition, leading to increased insurance
rates.
Similar issues arise at the state
level.
In 1999, California passed the
California Mental Health Parity Act to implement and extend
the federal MHPA.
In a landmark 2011 case (Harlick v. Blue Cross and Blue
Shield of California), the 9th Circuit Court of Appeals
ruled that health insurers must cover "medically
necessary" inpatient treatment -- not just outpatient
treatment -- for nine categories of "severe mental
illness": autism, bipolar disorder, (major) depression,
eating disorders, obsessive-compulsive disorder, panic
disorder, schizophrenia, schizoaffective disorder, and
"serious emotional disturbances" in children and
adolescents. Up until then, many insurers had refused to
cover inpatient treatment for these illnesses, favoring
less-expensive outpatient treatment instead. In fact, Ms.
Harlick's health-insurance policy did cover outpatient
treatment for mental illnesses, as well as short-term
inpatient treatment. But the 9th Circuit found that, in
many cases, long-term inpatient treatment was "medically
necessary", and so must be included in coverage to insure
that mental illnesses are covered to the same degree as
physical illnesses.
California is relatively progressive when it comes to
state funding of mental-health and substance-abuse
services. But the residents of other states may not
be so lucky. As noted earlier, the Republican
efforts to "repeal and replace" the Affordable Care Act
included provisions leaving it up to individual states to
determine the list of "essential" health-care services
that must be covered by any health insurance policy; and
among the most frequently mentioned candidates for removal
from that list were mental-health and substance-abuse
treatment.
Despite the movement toward parity, many
psychiatrists claim that they are not paid enough for their
services. As a result, they do not accept insurance, and
require that their patients pay out of pocket. A 2013
study by Bishop et al. (JAMA Psychiatry) found that
only 55% of psychiatrists accepted private insurance, compared
with 89% of other physicians, and only 55% of psychiatrists
accept Medicare patients, compared to 86% of other
specialists, and only 43% accept Medicaid patients, compared
to 73% of their colleagues. Whether these disparities
reflect a problem with reimbursement for mental-health
services, or the mendacity of some mental-health
professionals, isn't clear. mental-health. But it
makes clear that mental-health parity is only part of the
problem of delivering mental-health services. In
addition to balking at (allegedly) low payments, these
psychiatrists may also resist the kind of intrusive review
that comes with third-party payments. To be fair, many
psychiatrists are solo practitioners, and simply don't have
the office staff needed to cope with the paperwork that comes
with insurance -- and solo practitioners in all specialties
are less likely to take insurance than are physicians in any
sort of group practice. Then again, psychotherapy takes
time, and so long as insurers (including Medicare and
medicaid) reimburse on a fee-for-service basis,
psychotherapists will never be able to move as many patients
through their practice, or deliver as many services per unit
time, as other physicians (or, for that matter, psychiatrists
who do little more than dispense medication).
Perhaps for this reason, there aren't
enough psychiatrists and other mental-health professionals to
meet the demand. A 2012 study by the US Department of
health and Human Services found that fully 55% -- that's more
than half -- of the nation's 3100 counties have no practicing
psychiatrists, psychologists, or social workers.
And mental-health workers don't earn as
much as other medical professionals. A 2012 survey by
Medscape showed that the average income for psychiatrists is
only $186,000/year, ranking psychiatry 19th out of 25 medical
specialties. Now, $186,000 is not chump change -- but
it's not nearly as much as other physicians make.
So it's a system, and it can't be fixed
simply by mandating parity. Mental-health professionals
don't get paid enough, so there aren't enough of them.
Still, if psychotherapists could show
that what they do really works, then insurers would have
little choice but to pay for the services they deliver.
Which brings us to the most important feature of the current
mental-health environment, which is the move toward
evidence-based practices.
Evidence-Based Practice
But
these changes in mental-health policy and practice come with a
price, which is that, for the first time, mental-health
practitioners have to demonstrate that they know what they're
doing -- that their diagnoses are valid, and that their
treatments work.
Frankly, up until these changes in
policy, people didn't care much what went on in psychotherapy
-- largely because they weren't paying for it. People can do
what with their own money, the thinking went -- they can buy
cigarettes, or speedboats, or psychotherapy. But if they're
going to spend my money, whether in the form of
insurance premiums or taxes, they better be spending it on
something they really need, like a valid diagnosis, and
something that really works, like an effective treatment. And
also, frankly, "third-party" payers were still suspicious that
mental illness was a bogus concept, and psychotherapy a bogus
treatment. If people wanted to waste their own money on such
self-indulgence, that was fine. But they weren't going to
waste mine.
The upshot of all of this is that
mental-health parity was a huge boon for mental-health
practitioners, because they became eligible for third-party
payments from government and insurance companies -- not to
mention that parity also helped reduce the stigma of mental
illness. But parity came with a price -- which is that
mental-health practitioners actually had to prove, for the
first time, that their treatments actually worked.
But of
course, the very question of EBPs suggests that there are some
treatments that don't work, and some practices that aren't
empirically valid. Could this possibly be true?The simple,
straightforward answer is "Yes" -- but this is also true for
medicine in general, not just psychotherapy. The medical
profession has long cloaked itself with the mantle of science,
but until relatively recently physicians had relatively few
effective treatments for disease. Mostly, their treatments
were palliative in nature, intended to ameliorate the
patient's symptoms, and make the patient comfortable, while
nature took its course; or else they simply removed diseased
organs and tissues through surgery. Scientific medicine really
only began with the microbe-hunting of Louis Pasteur and
Robert Koch in the 19th century, and successive phases of the
pharmaceutical revolution of the 20th century. It is only
relatively recently that medical researchers have begun to
test medical practices to determine whether they actually
work, which ones work better than others, and which are cost
effective. Evidence-based medicine is epitomized by the
clinical trials that new drugs must go through, to demonstrate
their safety and efficacy, before they are marketed for the
treatment of specific diseases.
Something similar is now happening to
psychotherapy. For a long time, psychotherapists, including
psychiatrists and clinical social workers as well as clinical
psychologists, have had to operate "in the dark" about whether
their treatments were actually effective. Many
psychotherapists were loathe to measure the effects of their
treatments quantitatively. And so long as patients were paying
out of their own pockets, and so long as they believed
that they were being helped by their therapists, there was
little incentive for psychotherapists to validate their
practices scientifically. In the 20th century, as standards
for medical practice changed, psychotherapists felt under
increasing pressure to demonstrate that their practices, too,
"really worked". The pressure increased as responsibility for
paying for psychotherapy gradually shifted to "third parties"
(patients and their therapists were the first an second
parties) such as employers and health-insurance firms. These
third-party payees naturally want to make sure that they were
getting value for their money: and so they demanded that
psychotherapists, like other health professionals, show that
their practices were both effective and cost-effective.
Although there is an increasing literature on the validity of
various assessment practices, such as comparing "objective"
and "projective" techniques (see, e.g., "Clinical Assessment"
by J.M Wood, H.N. Garb, S.O. Lilienfeld, M.T. Nezworski,Annual
Review of Psychology, 2002), most practice research
focuses on treatment practices.
And, for that matter, something similar
is happening in other fields of public policy.
Under the Obama Administration, the federal Office of
Management and Budget has tried to promote experiments
structured like clinical trials, with random assignment of
subjects (or, for that matter, organizations) to conditions,
as a rational basis for policy changes. This trend is
most advanced in the field of education. Beginning with
the passage of the No Child Left behind Act during the George
W. Bush (43) Administration, the US Department of Education
has posted the findings of "clinical trials" of educational
innovations on its What
Works Clearinghouse website. Included among these
innovations are many of the teaching and learning strategies
discussed in the Exam Information
page.
Another name for evidence-based treatments is "empirically
supported treatment", or EST. The term "evidence-based
practice" (EBP) extends the scope of the EST movement to
procedures employed for diagnosis and assessment.
At
present, the standards for evidence-based practice in
psychotherapy are roughly modeled on the clinical trials
required before drugs are marketed (see, e.g., "Empirically
Supported Psychological Interventions: Controversies and
Evidence" by D.L. Chambless & T.H. Ollendick,Annual
Review of Psychology, 2001). In order to qualify as
"empirically supported", a treatment must yield outcomes that
are significantly better than those associated with an
adequate control (typically, patients who receive no treatment
at all) in at least two studies, preferably conducted by
independent research groups. An ongoing list of treatments
that meet current standards is maintained by Division 12
(Clinical Psychology) of the American Psychological
Association.
There
is a legitimate debate within and between the science and
clinical communities about what constitutes proper standards
for ESTs.
For example, some practitioners argue against any
standards at all, on the grounds that therapists should be
free to pick whatever treatment they think will be best
for the individual patient. Often they argue that
psychotherapy is an "art", not a science. But
physicians don't have this freedom: they have to conform
their practices to the available evidence -- and where
evidence is lacking, to the prevailing standard of
care. When physicians refer to the "medical arts",
they refer to the individual practitioner's skill -- but
even so, those "arts" are practiced within the bounds of
science.
Others, including some clinical scientists, believe
that the "efficacy" research that provides the basis for
ESTs is inappropriate, because the studies are conducted
under somewhat artificial conditions that do not represent
the problems that are encountered in actual practice.
Instead, they propose that ESTs be based on
"effectiveness" research, which they argue is more
"ecologically valid". But the distinction between efficacy
research and effectiveness research seems strained.
Research is research. Clinical drug trials are somewhat
artificial too, but their artificiality does not prevent
physicians from prescribing effective drugs in actual
practice. Moreover, "effectiveness" research often doesn't
seem to be very good research. In the highly touted Consumer
Reports study, for example, the outcome of
psychotherapy was measured by patients' self-reported
satisfaction with their treatment, instead of objective
evidence of actual improvement (see "The Effectiveness of
Psychotherapy: The Consumer Reports Study" by
M.E.P. Seligman,American Psychologist, December
1995; commentary on Seligman's article was published in
the October 1996 issue of the same journal. There were no
controls for sampling bias, nor any untreated control
group, for example. If the CR study is an example
of effectiveness research, then effectiveness research is
a step backward, not a step forward.
Still other practitioners hold that empirical evidence
of efficacy and effectiveness is only part of the equation
-- that the choice of treatment should also be based on
the clinician's expert judgment, and also on the patient's
values. While it's true that clinical expertise is
important, personal expertise should not trump scientific
evidence. An awful lot of common wisdom in mental health
proves, on examination, to be little more than folklore.
That is why physicians and surgeons rely on practice
guidelines, so that they can choose which of several empirically
valid treatments to recommend to their patients. And
while patients' values will help determine which treatment
they should receive, patient values don't trump empirical
evidence any more than clinical expertise does. A cancer
patient might want to be treated with avocado extract
instead of radiation and chemotherapy, and that's his
choice; but no third-party should be expected to pay for a
treatment that doesn't work.
Right
now, the standards for EST are pretty minimal. They are a good
start, but the standards need to be ratcheted up (the opposite
of dumbing down, I guess) over time to improve the quality of
psychotherapeutic practice.
For example, some might wish to drop no-treatment
control as an appropriate comparison group, in favor of an
appropriate placebo. And should a new treatment simply be
comparable to the available standard of care, or should it
somehow be better that what is available? These are the
same kinds of questions that are raised in drug research.
As another example, there is the matter of clinical vs.
statistical significance. A statistically significant
change in patient status may not be clinically significant
in terms of the ordinary course of everyday living. The
question is, what are the standards for clinical
significance?
As another example, two studies out of how many? The
current EST standard is modeled on current FDA standards,
which require only two positive trials, regardless of how
many negative or inconclusive trials there are, raising
the file-drawer problem and the issue of selective
publication of positive results.
As another example, and I think this is the really
interesting one, there is the question of mechanism. Since
the 19th century, medicine has generally rejected mere
"empirical" treatments, which are simply known to work, in
favor of treatments whose mechanisms of action can be
interpreted within the framework of existing knowledge of
anatomy and physiology. Not to say that new treatments
can't teach us something new about structure and function
(this is one of the reasons that people find hypnosis so
interesting), but you do expect a broad consistency. And
if a proposed treatment is inconsistent with what we
already know, that may be a reason to reject it regardless
of whether it works.
To take an example from the history of hypnosis (see
my paper in the International Journal of Clinical
& Experimental Hypnosis, October 2002),
Mesmer's animal magnetism wasn't rejected by the
Franklin Commission because it didn't work. Everyone
agreed that it did work. Animal magnetism was
rejected because Mesmer's theory was wrong, and nobody
had a good theory to replace it (psychology not having
been invented yet). Exorcism might work, empirically,
but even if it did medicine would reject it as a
legitimate treatment because its underlying theory --
that disease is caused by demon possession -- is
inconsistent with everything we know about how the body
works. In fact, Mesmer (and everyone else) agreed that
Fr. Gassner's exorcisms worked. But Mesmer won the
debate with Gassner because (at the time) he offered a
materialistic, and thus scientifically acceptable,
theory to account for his effects (the Franklin
Commission came along later).
It would represent a major "ratcheting
up" of the EST requirements if we required not just that the
treatment be efficacious, but that the theory on which the
treatment is based be scientifically valid as well. But it may
be exactly what we need (see below for more on this subject).
These are all points for debate within
the field. The actual standards for EST are the result of a
political process, and inevitably involve some compromise. But
once they are established, the important thing is that (1)
they are adhered to and (2) that if they are changed the
change is in the direction of tightening not loosening. If
practice is to be based on science, and science goes forward,
there can be no going back for practice.
It took a Supreme Court case, Virginia Academy of
Clinical Psychologists, and Robert J. Resnick, Ph.D. v.
Blue Shield of Virginia, (1977), to establish
psychologists' legal right to practice, and receive
reimbursement, without being supervised by psychiatrists or
other physicians. Clinical psychology owes is autonomy
from psychiatry, and its eligibility for third-party
payments, to the assumption that its practices rest on a
firm scientific foundation. Therefore, clinical psychology,
and the rest of the mental-health profession, departs from
scientific evidence at its own risk.
Putting Mental Illness in Social Context
Rosenhan's "pseudopatient"
study illustrates an important general point about mental
illness, and for that matter about normal mental and
behavioral functioning as well.
We assume (based on Chicago functionalism, described in
the lecture supplements on the Biological Bases of
Mind and Behavior) that the individual's mental life
takes place in a social context.
We know from the person-by-situation interaction
(described in the lecture supplement on Personality and Social
Interaction) that we cannot extricate the individual
from his or her surrounding social and cultural context.
What is true for normal mental
functioning is true for mental illness as well. We simply
cannot treat mental illness successfully by operating on the
individual alone. We must also act to change the social
environment in which the person lives.
For therapy to succeed,
mental-health professionals must do more than address the
individual's underlying psychopathology -- psychological
deficits, maladaptive social learning, diathesis and stress,
biological substrates, and so on.
They must also work with the patient's family members,
friends, neighbors, employers, and co-workers.
They -- and we -- must also work to change social
attitudes so that the mentally ill can live in an
environment that permits maximum recovery and adaptation.
When Will We Solve Mental
Illness?
Note:
On 11/19/2018, the New York Times
commemorated 40 years of its "Science Times"
section by looking at "11 Things We'd Really
Like to Know -- And A Few We'd Rather Not
Discuss". One of the essays, by
Benedict Carey, looked at progress in
understanding the causes and treatment of
mental illness. Note the downplaying
of biology, and the underscoring of the role
of experience -- even by biological
psychiatrists!
Biology was supposed to cure what ails
psychiatry. Decades later, millions of
people with mental disorders are still
waiting.
Nothing
humbles history’s great thinkers more
quickly than reading their declarations on
the causes of madness. Over the centuries,
mental illness has been attributed to
everything from a “badness of spirit”
(Aristotle) and a “humoral imbalance”
(Galen) to autoerotic fixation (Freud) and
the weakness of the hierarchical state of
the ego (Jung).
The arrival of
biological psychiatry, in the past few
decades, was expected to clarify matters, by
detailing how abnormalities in the brain
gave rise to all variety of mental distress.
But that goal hasn’t been achieved — nor is
it likely to be, in this lifetime.
Still, the
futility of the effort promises to inspire a
change in the culture of behavioral science
in the coming decades. The way forward will
require a closer collaboration between
scientists and the individuals they’re
trying to understand, a mutual endeavor
based on a shared appreciation of where the
science stands, and why it hasn’t progressed
further.
“There has to
be far more give and take between
researchers and the people suffering with
these disorders,” said Dr. Steven Hyman,
director of the Stanley Center for
Psychiatric Research at the Broad Institute
of M.I.T. and Harvard. “The research cannot
happen without them, and they need to be
convinced it’s promising.”
The course of
Science Times coincides almost exactly with
the tear-down and rebuilding of psychiatry.
Over the past 40 years, the field remade
itself from the inside out, radically
altering how researchers and the public
talked about the root causes of persistent
mental distress.
The blueprint
for reassembly was the revision in 1980 of
psychiatry’s field guide, the Diagnostic and
Statistical Manual of Mental Disorders,
which effectively excluded psychological
explanations.
Gone was the rich Freudian language
about hidden conflicts, along with the
empty theories about incorrect or
insufficient “mothering.” Depression
became a cluster of symptoms and
behaviors; so did obsessive-compulsive
disorder, bipolar disorder, schizophrenia,
autism and the rest.
This
modernized edifice struck many therapists as
a behavioral McMansion: an eyesore, crude
and grandiose. But there was no denying that
the plumbing worked, the lighting was
better, and the occupants had a clear,
agreed-upon language.
Researchers
now had tidier labels to work with; more
sophisticated tools, including M.R.I.s,
animal models, and genetic analysis, to
guide their investigations of the brain; and
a better understanding of why the available
drugs and forms of psychotherapy relieved
symptoms for many patients.
Science journalists, and their readers, also had
an easier time understanding the new vocabulary.
In time, mental problems became mental disorders,
then brain disorders, perhaps caused by faulty
wiring, a “chemical imbalance” or genes.
But the actual
science didn’t back up those interpretations.
Despite billions of dollars in research
funding, and thousands of journal articles,
biological psychiatry has given doctors and
patients little of practical value, never mind
a cause or a cure.
Nonetheless,
that failure offers two valuable guideposts
for the next 40 years of research.
One is that
psychiatry’s now-standard diagnostic system —
the well-lighted structure, with all its
labels — does not map well onto any shared
biology. Depression is not one ailment but
many, expressing different faces in different
people. Likewise for persistent anxiety,
post-traumatic stress, and personality issues
such as borderline personality disorder.
As a result, the
best place for biological scientists to find
traction is with individuals who have highly
heritable, narrowly defined problems. This
research area has run into many blind alleys,
but there are promising leads.
In 2016,
researchers at the Broad Institute found
strong evidence that the development of
schizophrenia is tied to genes that regulate synaptic
pruning, a natural process of brain
reorganization that ramps up during
adolescence and young adulthood.
“We are now
following up hard on that finding,” said Dr.
Hyman. “We owe it those who are suffering with
this diagnosis.”
Scientists
also foresee a breakthrough in understanding
the genetics of autism. Dr. Matthew State,
chief of psychiatry at the University of
California, San Francisco, said that in a
subset of people on the autism spectrum,
“the top 10 associated genes have huge
effects, so a clinical trial using gene
therapies is in plausible reach.”
The second
guidepost concerns the impact of biology.
Although there
are several important exceptions, measurable
differences in brain biology appear to
contribute only a fraction of added risk for
developing persistent mental problems.
Genetic inheritance surely plays a role, but
it falls well short of a stand-alone “cause”
in most people who receive a diagnosis.
The remainder
of the risk is supplied by experience: the
messy combination of trauma, substance use,
loss and identity crises that make up an
individual’s intimate, personal history.
Biology has nothing to say about those
factors, but people do. Millions of
individuals who develop a disabling mental
illness either recover entirely or learn
to manage their distress in ways that
give them back a full life. Together, they
constitute a deep reservoir of scientific
data that until recently has not been
tapped.
Gail
Hornstein, a professor of psychology at
Mount Holyoke College, is now running a
study of people who attend meetings of the Hearing
Voices Network, a grass-roots,
Alcoholics Anonymous-like group where people
can talk with one another about their mental
health struggles.
Many
participants are veterans of the psychiatric
system, people who have received multiple
diagnoses and decided to leave medical care
behind. The study will analyze their
experiences, their personal techniques to
manage distress, and the distinctive
characteristics of the Hearing Voices groups
that account for their effectiveness.
“When people
have an opportunity to engage in ongoing,
in-depth conversation with others with
similar experiences, their lives are
transformed,” said Dr. Hornstein, who has
chronicled the network and its growth in the
United States. “We start with a person’s own
framework of understanding and move from
there.”
She added: “We
have underestimated the power of social
interactions. We see people who’ve been in
the system for years, on every med there is.
How is it possible that such people have
recovered, through the process of talking
with others? How has that occurred? That is
the question we need to answer.”
To push beyond
the futility of the last 40 years,
scientists will need to work not only from
the bottom up, with genetics, but also from
the top down, guided by individuals who have
struggled with mental illness and come out
the other side.
Their
expertise is fraught with the pain of having
been misunderstood and, often, mistreated.
But it’s also the kind of expertise that
researchers will need if they hope to build
a science that even remotely describes, much
less predicts, the fullness of human mental
suffering.