![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
The Arizona Motor Scale of Hypnotizability (AMSH) is so named because it focuses on ideomotor suggestions within the domain of hypnosis (Hilgard, 1965; Kihlstrom, 2008). It was originally developed at the University of Arizona to explore the distinction between "direct" and "challenge" suggestions in the factor structure of hypnosis. It was also employed in a pilot study of hypnotizability in brain-damaged patients.
The AMSH was never intended for general use, or as a substitute for the scales traditionally employed in hypnosis research, such as the Harvard Group Scale of Hypnotic Susceptibility, Form A (HGSHS:A), and the Stanford Hypnotic Susceptibility Scales, Form A (SHSS:A) and Form C (SHSS:C). For this reason, I have hesitated to publish the AMSH itself in any form.
The purpose of this paper is simply to document the procedure, in support of the two studies in which it was used.
The AMSH consists of an induction of hypnosis by eye closure, taken verbatim from the SHSS:A. This is followed by a series of representative hypnotic suggestions, each of which is scored according to an objective behavioral criterion of response. Most of these suggestions were drawn from the SHSS:A, SHSS:C, or HGSHS:A (HGSHS:A is a close adaptation of SHSS:A for group administration); a few were devised anew, taking the established suggestions as models. Although the focus of AMSH was on ideomotor suggestions (hence its name), three items representing the cognitive factor were also included, so that scores resembling those of SHSS:A or HGSHS:A could be derived.
Table 1 shows the items of AMSH, their source, and their assignment to the three major factors of hypnotizability: direct suggestion (Dir), challenge suggestion (Cha), and cognitive alteration (Cog).
Table 1 |
||
Items of the Arizona Motor Scale of Hypnotizability |
||
Item |
Source (Item#)* |
Factor |
01. Eye Closure |
SHSS:A (2) | Dir |
02. Hand Lowering |
SHSS:A (3) | Dir |
03. Arm Immobilization |
SHSS:A (4) | Cha |
04. Head Shaking |
HGSHS:A (8) | Cha |
05. Hands Moving Apart |
SHSS:B (7) | Dir |
06. Finger Lock |
SHSS:A (5) | Cha |
07. Arm Rigidity |
SHSS:A (6) | Cha |
08. Head Falling |
HGSHS:A (1) | Dir |
09. Verbal Inhibition |
SHSS:A (8) | Cha |
10. Hand Levitation |
New | Dir |
11. Arms Lowering |
New | Dir |
12. Mosquito Hallucination |
SHSS:C (9) | Cog |
13. Eye Catalepsy |
SHSS:A (10) | Cha |
14. Hands Moving Together |
SHSS:A (7) | Dir |
15. Posthypnotic Suggestion |
HGSHS:A (11) | Cog |
16. Posthypnotic Amnesia |
SHSS:A (12) | Cog |
| *Parentheses indicate the item number in the standardized scale from which the AMSH item was derived. The "new" items #10 and 11 were modeled after Item #02, "Hand Lowering" | ||
As in the standardized scales on which it was based, the subject's response to each suggestion is scored according to objective behavioral criteria. In contrast to their dichotomous scoring, however, AMSH allows these responses to be scored on a continuous scale: the experimenter simply records whether the subject met the behavioral criterion of response, and the segment of the script in which he or she did so. Accordingly, the text of each suggestion was divided into segments so as to yield a 9-point scale (0-8). For some items, the interval allotted for a positive response was extended from 10 to 20 seconds, in anticipation of the compromised abilities of brain-damaged patients.
For example:
| On Item #02, Hand Lowering, a direct suggestion, subjects whose outstretched hands lowered at least 6 inches during the first segment of text received a full score of 8; those whose hands had not fallen that distance, even after a 20-second interval of silence had elapsed at the end of the suggestion, received a score of 0. | |||||||||||||
| On Item #03, Arm Immobilization, a challenge suggestion, subjects whose arms bent more than 2 inches during the first segment of text received a score of 0, while those whose arm had not bent this amount even after a 20-second interval had elapsed at the end of the suggestion received a full score of 8. | |||||||||||||
| On Item #12, Mosquito Hallucination, a cognitive suggestion, subjects who made some outward acknowledgement of the insect as soon as it was mentioned received a full score of 8; those who did not acknowledge its presence at all, even after a 20-second interval had lapsed, received a score of 0. | |||||||||||||
| In principle, Item #15, Posthypnotic Suggestion, another cognitive suggestion, could be scored in terms of the latency of response after administration of the cue, but this proved difficult to manage in practice. Instead, subjects received a full 8 points if they responded to the cue (most did so immediately), or 0 points if they did not respond at all. | |||||||||||||
Continuous scoring of
Item #16, Posthypnotic Amnesia, the third cognitive
suggestion, admitted a number of ways to take account of
both initial amnesia and subsequent reversibility
(Kihlstrom & Register, 1984). After
experimenting with a number of different combinations of
initial amnesia and reversibility, we settled on the
following scheme (other schemes are perfectly defensible):
|
The reversed scoring of direct and challenge suggestions is due to differences in the nature of these two types of ideomotor suggestions: subjects pass direct suggestions by displaying the observed response (e.g., by their outstretched hand lowering quickly after it is suggested that it is too heavy to hold up); challenge suggestions are passed by failing to do so (e.g., by failing to bend the arm after it is suggested that it is too rigid to bend).
Further details of individual item scoring are available in the AMSH script.
Because of their derivation from published scales, the characteristics of most of the individual AMSH items are well known (e.g., Hilgard, 1965). In addition, some normative data was provided by a group of 100 college students who volunteered for an experiment on hypnosis as part of the research participation component of their introductory psychology course.
This group was composed of 39 men and 61 women aged 18-30 (M = 20.69, SD = 2.38) -- a gender distribution that resembled that of the subject pool as a whole.
 With 16 items, each scored on a 9-point
scale (0-8), continuous scores on the AMSH can vary from a low
of 0 to a high of 128.
With 16 items, each scored on a 9-point
scale (0-8), continuous scores on the AMSH can vary from a low
of 0 to a high of 128.
| Scores on the AMSH ranged from a low of 25 to a high of 105: M = 62.08, SD = 19.42. The median score was 60.5. | |
| Aggregating scores by decade, the distribution of scale scores appeared to be bimodal, with modes appearing in the 40-49 and 60-69 ranges. | |
| The reliability of the scale, as determined by Cronbach's alpha, was .86. | |
| The median corrected item-to-total correlation was .50 (range: .25-.68). |
Table 2 shows the individual item analysis.
Table 2 |
||
Item Analysis: Continuous Scores |
||
Item |
M Score |
Item-to-Total r |
01. Eye Closure |
2.99 | .25 |
02. Hand Lowering |
3.99 | .43 |
03. Arm Immobilization |
4.65 | .41 |
04. Head Shaking |
4.14 | .42 |
05. Hands Moving Apart |
4.10 | .57 |
06. Finger Lock |
5.85 | .68 |
07. Arm Rigidity |
5.65 | .57 |
08. Head Falling |
3.81 | .66 |
09. Verbal Inhibition |
4.60 | .47 |
10. Hand Levitation |
2.31 | .68 |
11. Arms Lowering |
4.20 | .51 |
12. Mosquito Hallucination |
1.60 | .45 |
13. Eye Catalepsy |
5.09 | .52 |
14. Hands Moving Together |
3.04 | .51 |
15. Posthypnotic Suggestion |
3.15 | .47 |
16. Posthypnotic Amnesia |
2.92 | .49 |
| *Segment of script in which subject met the standard criterion for passing the item. | ||
 Each of the scale items could also be
scored dichotomously, by applying the standardized scoring
criteria specified in the scales from which the items were drawn
(scoring criteria for the new items #10-11 were derived by
analogy from Item #02).
Each of the scale items could also be
scored dichotomously, by applying the standardized scoring
criteria specified in the scales from which the items were drawn
(scoring criteria for the new items #10-11 were derived by
analogy from Item #02).
| These scores ranged from 0 to 16: M = 8.56, SD = 3.63. The median score was 8.0. | |
| Again, the distribution of scale scores appeared to be bimodal. | |
| The reliability of the scale, as determined by coefficient alpha, was .85. | |
| The median corrected item-to-total correlation was .50 (range: .14-.69). |
Table 3 shows the item analysis.
Table 3 |
||
Item Analysis: Applying Standard Criteria |
||
Item |
Criterion* |
% Passing |
01. Eye Closure |
3 | 89 |
02. Hand Lowering |
5 | 95 |
03. Arm Immobilization |
5 | 23 |
04. Head Shaking |
4 | 12 |
05. Hands Moving Apart |
5 | 84 |
06. Finger Lock |
6 | 72 |
07. Arm Rigidity |
6 | 46 |
08. Head Falling |
5 | 72 |
09. Verbal Inhibition |
5 | 19 |
10. Hand Levitation |
1 | 43 |
11. Arms Lowering |
5 | 94 |
12. Mosquito Hallucination |
2 | 38 |
13. Eye Catalepsy |
5 | 32 |
14. Hands Moving Together |
4 | 59 |
15. Posthypnotic Suggestion |
1 | 39 |
16. Posthypnotic Amnesia |
2 | 39 |
| *Lower limit of continuous score required for a "pass". | ||
The AMSH can also be scored by considering only those 12 items that appear on SHSS:A or HGSHS:A, thus yielding scores that are comparable to what would have been obtained with those standardized scales. These scores were calculated as the sum of items #01-03, 06-09, and 12-16.
However, these minor differences between AMSH and the standard scales should be noted:
| Item #09, Verbal Inhibition, appears on the individually administered SHSS:A; the comparable item on the group-administered HGSHS:A is #04, "Head Shaking". | |
| Both SHSS:A and HGSHS:A have a "Fly Hallucination" item; AMSH employs the "Mosquito Hallucination" item from SHSS:C instead. | |
| SHSS:A has a "Postural Sway" item as a test of "waking" ideomotor suggestibility, administered before the induction of hypnosis. The comparable item of HGSHS:A is "Head Falling Forward". AMSH omits any test of nonhypnotic response to suggestion, but includes the HGSHS:A "Head Falling" as Item #08, administered during hypnosis. |
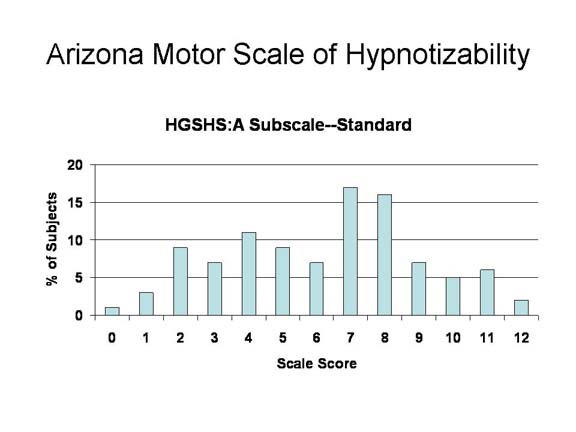 When the 12 "Form
A" items were scored according to the standard criteria, the
mean score of 6.23 (SD = 2.86) was comparable to that of
SHSS:A or HGSHS:A.
When the 12 "Form
A" items were scored according to the standard criteria, the
mean score of 6.23 (SD = 2.86) was comparable to that of
SHSS:A or HGSHS:A.
| The median score was 7.0. | |
| Again, the distribution of scale scores appeared to be bimodal. | |
| The reliability of the scale, as determined by coefficient alpha, was .78. | |
| The median corrected item-to-total correlation was .40 (range: .16-.59). |
The correlation between the full 16-item AMSH and the 12-item "Form A" subscale was r = .98 p < .001).
As noted earlier, the primary motive for constructing the AMSH was to address a controversy over the factorial structure of hypnosis, particularly with respect to the direct and challenge suggestions within the ideomotor domain. Factor analyses of the standard hypnotizability scales, such as SHSS:A and HGSHS:A, routinely yield three factors, identified as direct, challenge, and cognitive suggestions.
As expected, as is clear from Table 3, these three types of items differ significantly in terms of difficulty level.
| The average pass rate for the 6 direct suggestions (omitting #01, Eye Closure, which is administered during the hypnotic induction itself) was 74.50%, compared to 34.00% for the 6 challenge suggestions and 38.67% for the 3 cognitive suggestions. | |
| The mean score for the 6 direct suggestions was 4.47 (SD = 1.55), compared to a mean of 2.04 (SD = 1.78) for the 6 challenge suggestions. The difference is highly significant: t(99) = 14.43, p , .001. |
This empirical fact, in turn, raises the possibility that the underlying factor structure itself is an artifact of item difficulty (Coe & Sarbin, 1971).
One way to address this issue is to factor-analyze continuous item scores.
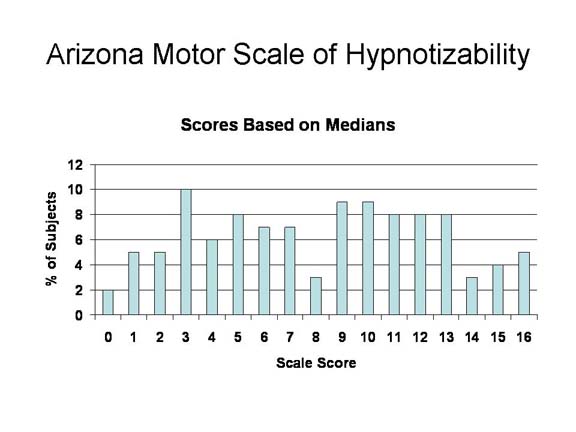 Another
approach
is to establish alternate dichotomous criteria that equate, as
closely as possible, the difficulty levels of the various
items. To this end, we inspected the distribution of
continuous scores for each of the items, and established a
cutpoint that, as closely as possible, divided this distribution
in half. It was not always possible to obtain a precise
50-50 split, but in the end the average pass percent for the 6
direct suggestions was 49.33, compared to 45.83 for the
challenge suggestions and 44.00 for the 3 cognitive
suggestions. Put bluntly, with these new cutpoints, the
direct suggestions were made harder, and the challenge and
cognitive suggestions were made easier.
Another
approach
is to establish alternate dichotomous criteria that equate, as
closely as possible, the difficulty levels of the various
items. To this end, we inspected the distribution of
continuous scores for each of the items, and established a
cutpoint that, as closely as possible, divided this distribution
in half. It was not always possible to obtain a precise
50-50 split, but in the end the average pass percent for the 6
direct suggestions was 49.33, compared to 45.83 for the
challenge suggestions and 44.00 for the 3 cognitive
suggestions. Put bluntly, with these new cutpoints, the
direct suggestions were made harder, and the challenge and
cognitive suggestions were made easier.
| With this alternative scoring procedure, Scores on the AMSH ranged from a low of 25 to a high of 90: M = 55.75, SD = 15.33. The median score was 56.6. | |
| Aggregating scores by decade, the distribution of scale scores appeared to be bimodal, with modes appearing in the 40-49 and 60-69 ranges. | |
| The reliability of the scale, as determined by coefficient alpha, was .83. | |
| The median corrected item-to-total correlation was .46 (range: .21-.65). |
Table 4 shows the item analysis.
Table 4 |
||
Item Analysis: Applying "Median Split" Criteria |
||
Item |
Criterion* |
% Passing |
01. Eye Closure |
2 | 56 |
02. Hand Lowering |
2 | 29 |
03. Arm Immobilization |
6 | 35 |
04. Head Shaking |
6 | 70 |
05. Hands Moving Apart |
3 | 66 |
06. Finger Lock |
5 | 48 |
07. Arm Rigidity |
6 | 46 |
08. Head Falling |
3 | 60 |
09. Verbal Inhibition |
6 | 30 |
10. Hand Levitation |
3 | 48 |
11. Arms Lowering |
2 | 46 |
12. Mosquito Hallucination |
2 | 38 |
13. Eye Catalepsy |
6 | 46 |
14. Hands Moving Together |
3 | 47 |
15. Posthypnotic Suggestion |
5 | 40 |
16. Posthypnotic Amnesia |
3 | 54 |
| *Lower limit of continuous score required for a "pass". | ||
This strategy was fairly successful in equating item difficulties:
| The average pass rate for the 6 direct suggestions (omitting #01, Eye Closure, which is administered during the hypnotic induction itself) was 49.33%, compared to 45.83% for the 6 challenge suggestions and 44.00% for the 3 cognitive suggestions. | |
| The mean score for the 6 direct suggestions was 2.96 (SD = 1.91), compared to a mean of 2.75 (SD = 1.91) for the 6 challenge suggestions. The difference is not statistically significant: t(99) = 11.17. |
The correlation between the "standard" and "median split" scorings of the full AMSH was r = .93 (p < .001).
The Arizona Motor Scale of Hypnotizability has excellent psychometric properties -- both in comparison to existing scales, such as SHSS:A and HGSHS:A, and to psychometric instruments in general, with reliability (coefficient alpha) well into the "good" range, and individual item-to-total correlations generally high.
However, the AMSH is not recommended for general use. One of the most important milestones in hypnosis research was the availability of objective, standardized scales for measuring hypnotizability, such as the Stanford and Harvard scales. Their widespread adoption helped insure that different hypnosis laboratories assessed hypnotizability in the same way, and was the key to the scientific acceptability of the field. Any proliferation of alternative hypnotizability scales (as has, unfortunately, already begun to occur) compromises this situation, works to the detriment of hypnosis research in general.
On occasion, it is appropriate to devise new hypnotizability scales for specialized purposes, as in this case. But the "gold standard" for the assessment of hypnotizability remains the a group administration of HGSHS:A followed by an individual administration of SHSS:C.
Coe, W. C., & Sarbin, T. R. (1971). An alternative interpretation to the multiple composition of hypnotic scales: A single role-relevant skill. Journal of Personality and Social Psychology, 18, 1-8.
Hilgard, E. R. (1965). Hypnotic susceptibility. New York: Harcourt, Brace, & World.
Kihlstrom, J. F. (2008). The domain of hypnosis, revisited. In M. Nash & A. Barnier (Eds.), Oxford handbook of hypnosis (pp. 21-52). Oxford: Oxford University Press.
Kihlstrom, J. F., & Register, P. A. (1984). Optimal scoring of amnesia on the Harvard Group Scale of Hypnotic Susceptibility, Form A. International Journal of Clinical & Experimental Hypnosis, 32(1), 51-57.
This page last revised 12/22/2011.