Final Examination
Narrative Review
Click here for general information about exams in this course.
The Exam
The date for the final exam is given in the Syllabus and Calendar on Canvas.
- A second sitting has been scheduled for students with
conflicting final exams. If you have such a conflict, you
should consult with both the instructors involved to
resolve it. Students in this situation should contact
me no later than two (2) weeks prior to the scheduled final
exam.
- Students in the DSP program will be notified of arrangements for their exams.
There are lots of resources available for the examination. In addition to this narrative review, there are lots of materials on the course website: the Lecture Supplements, which contain expanded treatment of the lectures given in class, as well as copies of all past exams, with answers (and usually with explanations of the answers). I don't intentionally repeat questions from year to year, but the topics I deem important don't change that much.
In addition, students are encouraged to post questions to the Queries and Comments module of the course website on Canvas. Either I or the GSIs will do our best to respond to them, provided that they are posted no later than noon on the day before the exam. Do not send questions by private Email to either me or the GSIs: we want to make sure that everybody in class has equal access to the exchanges.
The exam will consist of 100 multiple-choice questions. Roughly half will be drawn directly from the lectures, roughly half will be drawn directly from the text. Of course, there is some overlap between lectures and readings.
Roughly 1/4of the exam (approximately 25 items) will be noncumulative, with questions drawn from lectures and readings assigned since the last exam. The remaining 3/4 (roughly) will be cumulative, with questions drawn from the entire course.
The exam will be computer scored according to procedures outlined in the Exam Information page on the course website.
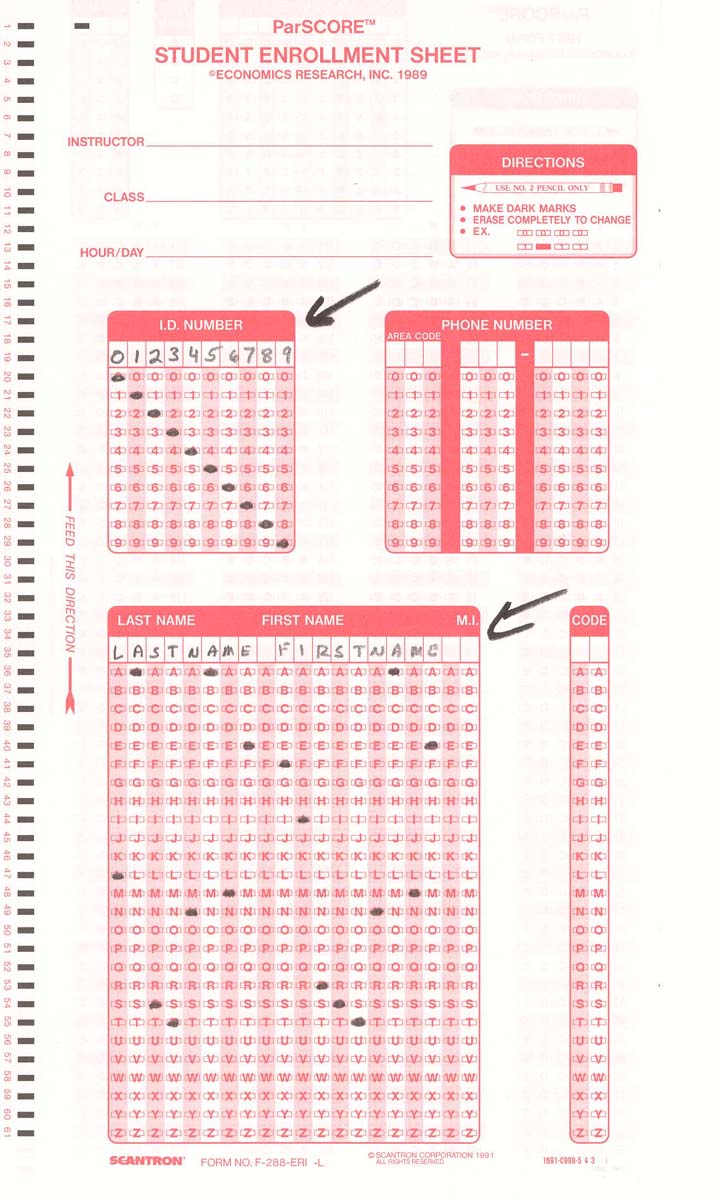
The Scantron Form
 For purposes of
recording your answers, you should purchase several copies of
the red Scantron form (pictured at the left), as well as
several #2 pencils. Scantron forms are available at the ASUC
Bookstore and at other outlets in and around campus.
For purposes of
recording your answers, you should purchase several copies of
the red Scantron form (pictured at the left), as well as
several #2 pencils. Scantron forms are available at the ASUC
Bookstore and at other outlets in and around campus.
Be sure you purchase the proper Scantron form, known as the ParSCORE Form No. F-288-ERI-L. Sometimes the vendor changes the exact "Form No." on us, but:
- The proper Scantron form looks like the illustrations here.
- And it is red.
Scantron forms cannot be completed in ink.
Here's how to fill out the Scantron form:
|
|
On the front side of the Scantron form, fill in your eight-digit UCB Student ID number. Use the first eight (8) columns for this purpose. Do not use leading zeros (0s). Fill in the bubbles accordingly. Then fill in your name, last name first, and fill in the bubbles accordingly. You do not have to fill in any other spaces on this side of the Scantron form. You don't have to fill in the Instructor, or the Class, or the Hour/Day. We don't want your phone number. There is no Code. |
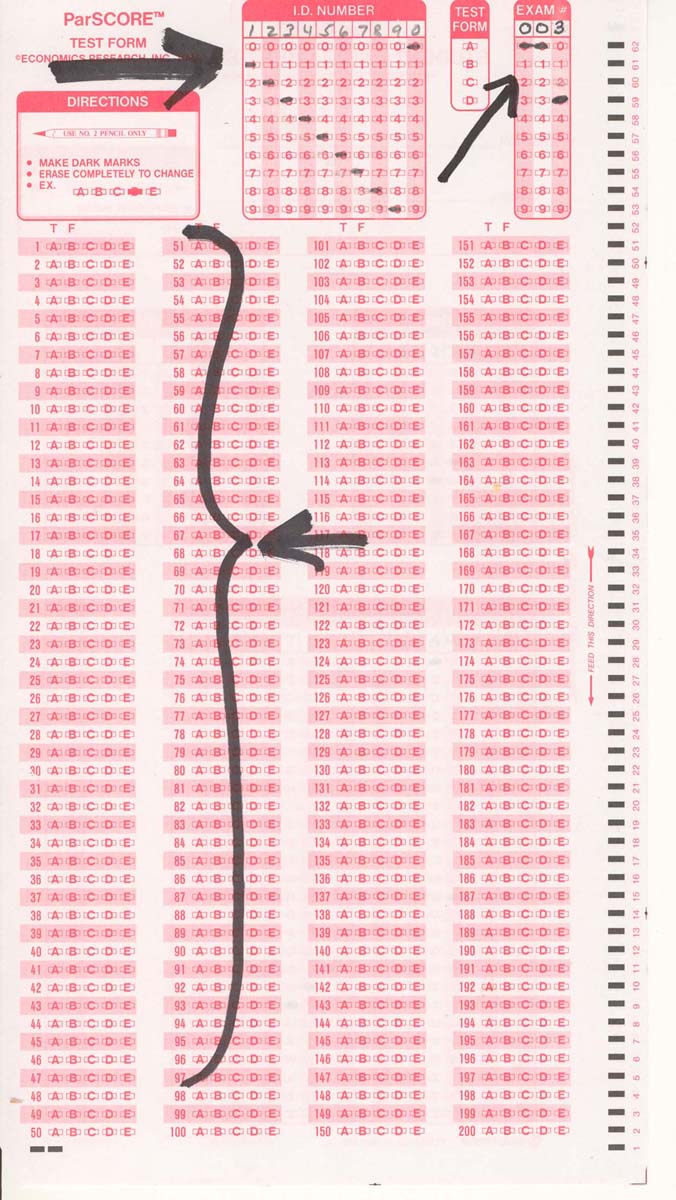
|
|
On the reverse side of the Scantron form, fill in your eight-digit UCB Student ID number, and bubble in, as before -- no leading zeroes. Under Exam #, fill in 003, with two leading zeroes, and bubble in. There is only one form of the test, so leave Test Form blank. Then fill in your answers to the 100 questions in the two left columns (#s 1-100). |
Exam Construction and Scoring
The focus of my exam is on basic concepts and principles. There are no questions about names or dates (though names and dates may appear in questions). There are no questions about picky details. There are no questions about specific experiments, though you should be able to recognize the implications of the phenomena revealed by some classic experiments. There are no intentionally tricky questions: I want you to understand basic concepts and principles, not the exceptions to the rules.
The exam will be scored twice, following the procedures outlined in the page on Exam Information. Usually, we try to post exam grades within a couple of days of the exam. In the meantime, be sure to save your exam, with a record of your answers. That way, you'll be able to check your answers against the preliminary and revised scoring keys, as they are posted (wait for an announcement via Email, and posted to the website).
When grades are posted, there will also be an announcement to this effect, and then students will have a brief opportunity to correct any errors that may have occurred in the grading. At Berkeley, final grades are due within 96 hours of the final exam.
Psychological Development
There are three different views of
development: ontogenetic, phylogenetic, and culture. Both the
lectures and the textbook emphasize the ontogenetic view,
which has to do with the development of mind and behavior in
the individual. Psychology emphasizes the ontogenetic
view, tough the phylogenetic and cultural views are not
unimportant.
The lectures focused on the
"nature-nurture" issue, and particularly the interaction of
nature and nurture, as represented by the way in which the
individual's genotype interacts with the environment
(prenatal, perinatal, and postnatal) to produce a phenotype.
The nature-nurture issue resembles the conflict between nativist and empiricist views of knowledge: to what extent are aspects of mind and behavior innate, and to what extent are they acquired through experience? One extreme view of "nature", and of nativism, is an emphasis on differentiation and maturation of the individual, which seems to portray development as something that happens to the individual. But the lectures, and for that matter, the text as well, portray the individual as taking a more active role as an agent of his or her own development.
You should understand the various types
of shared environment, and why we consider them to be "shared"
among siblings. And you should understand the various
kinds of nonshared environment, and why we consider them to be
"nonshared".
The lectures focused on the interaction of nature and nurture in personality development, as reflected in the results of research using the twin study method. You should understand the logic of the twin study, that to the extent that a trait is inherited, monozygotic twins will be more similar on that dimension than dizygotic twins. You needn't memorize the formulas for estimating the contributions of genetics, the shared environment, and the nonshared environment, but you should understand these three concepts, and you should know that anything less than 100% similarity between MZ twins is evidence for the role of the nonshared environment.
- You definitely should know that, in almost all cases, genetic factors account for no more than 50% of population variance on psychological variables (like personality).
- And that the nonshared environment usually accounts for the vast bulk of the environmental contribution to variance.
- And, for that matter, that the contribution of the
nonshared environment usually matches that of the genes.
It turns out that the role of the nonshared environment (within-family differences) is big indeed, which is why I say that, psychologically speaking, each child is born to different parents, raised in a different family, lives in a different neighborhood, attends a different school, and worships in a different church. You should understand the sources of within-family differences, especially child-driven effects, relationship-driven effects, parent-driven effects, and family context effects. And you should be able to recognize examples of each of the different kinds of effects.
I presented some research on birth-order effects on personality and intelligence to illustrate the effects of family micro-environments. Zajonc's confluence model is an interesting (and provocative) example of the general point that each child is both shaped by its family environment, and also reciprocally shapes that environment in turn. So you should understand the basics of the model:
- The dilution and growth effects.
- The teaching effect and the last-child and only-child handicaps.
- The effects of spacing, family size, multiple births, single parents, and extended families.
The lecture on gender dimorphism was intended to illustrate the interaction of biological and environmental factors on critical aspects of personality development -- namely, gender identity, gender role, and sexual orientation.
- You should understand how, according to Money and Ehrhardt, the program for gender dimorphism unfolds.
- What it means to "add something to masculinize".
- You don't have to know the precise timing of the development of the male and female internal and external genitalia (this isn't a biology course), but you should get the general idea about how fetal gender dimorphism can produce the various forms of male and female pseudohermaphroditism.
- You should understand the traditional (Western) gender roles of agency and communality.
- And how they can combine to produce traits like psychological androgyny.
- And the results of twin studies on the development of individual differences in masculinity and femininity.
- How, beginning at about age 2, the child begins to recognize his or her own gender, and starts to take an active role in psychosexual development.
- The implications of twin studies for understanding the origins of of homosexuality.
The final lecture applied many of these points to cognitive development.
- The idea of development as continuous change is exemplified by Gesell's work on maturation, and the concept of IQ.
- Piaget offered an alternative view of development as consisting of a sequence of more-or-lesss discrete changes.
- You should recognize Piaget's stages and their corresponding landmarks.
- Sensory-motor intelligence and object permanance
- The pre-operational epriod and conservation
- Concrete operations and egocentrism.
- Formal operations and abstract thought.
- You should understand how the basic idea of developmental stages was adopted by other developmental theorists.
- Of particular interest are Erikson's "eight ages of man" and Kohlberg's stages of moral development.
- No, you don't have to memorize all eight of
Erikson's stages. But
- it might help to know that adolescence is characterized by "identity vs. role confusion"!
- You should understand the problems with Piaget's theory, especially the finding that the lower boundaries of his stages are quite flexible, depending on how children are tested.
- For example, the child's understanding of number.
- And the discovery that even infants can do simple arithmetic.
- Development as the acquisition of expertise.
- And differences between "expert" and "novice" cognition.
- Development as the acquisition of metacognition, which lays the groundwork for...
- Development as the development of a theory of mind,
- including the rationale for the "false belief" task
- ...which lays the ground for the "theory theory" of cognitive development.
- Which brings us back to the idea of development as learning, viewed as the active generation, testing, and refinement of theories about oneself and the world.
Chapter 5
The lectures on development come
relatively late in the course, though Kalat discusses them
early in his book.
The chapter begins with methods for studying psychological development, and you should understand the difference between cross-sectional and longitudinal designs, and the advantages and disadvantages of each (e.g., cohort effects).
With respect to physical development, you should understand:
- The stages of prenatal development, from the zygote to the fetus, including the effects of alcohol on fetal development -- especially of the nervous system.
- Visual perception in infancy, especially with respect to faces.
- Hearing in infancy, especially the use of habituation paradigms to study their ability to distinguish syllables such as ba and pa.
- The use of habituation paradigms to study learning and memory.
There is a nice summary of Piaget's stage theory of cognitive development. You should be able to characterize the different stages, and the landmarks associated with them:
- Sensorimotor stage (object permanence).
- Preoperational stage (egocentrism).
- Concrete operations (conservation).
- Formal operations (logical reasoning).
You should also understand some of the problems with Piaget's theory, especially the question of whether the Piagetian stages are as distinct as Piaget thought they were.
You should understand Vygotsky's concept of the "zone of
proximal development".
Kalat discusses the "Theory of Mind" in his section on Piaget, and you should understand the connection between Piaget's concept of egocentrism and the acquisition of a theory of mind.
- Understanding false beliefs.
- Distinguishing appearance from reality.
Kalat's discussion of socio-emotional development focuses on
Erik Erikson's stage theory, and you should understand the
basic conflicts that, Erikson thought, characterized each of
his "eight ages of man".
There are also other important topics:
- Attachment styles in infancy and childhood, as revealed in the Strange Situation: secure, anxious, avoidant, and disorganized.
- Individual differences in temperament.
- Risk-taking, peer pressure, and identity in adolescence.
- Midlife transitions in adulthood.
- Life satisfaction and "terror management" in old age.
Although we often think of development as a kind of universal unfolding of adult mind and personality, there is considerable diversity in the paths that development can take. You should know about some of these differences and their sources:
- Gender differences in spatial ability and sex roles (and their roots in experience as well as biology).
- Differences between "individualistic" and "collectivist" cultures, and the effects of biculturalism.
- Effects of birth order and family size on IQ.
- Parenting styles: authoritative, authoritarian (they're different), permissive, and indifferent.
- Nontraditional families, including the effects of divorce, and comparisons of traditional and single-parent households.
Consciousness
Once we've covered the basics of cognition -- sensation and perception, attention and memory, thinking and language -- we're ready to put it all together and try to figure out what consciousness is all about.Ordinarily, I'd prefer to discuss consciousness, and unconscious mental life, as part of the lectures on "The Trilogy of Mind" -- thinking, feeling, and desiring are, after all, conscious mental states, and it's an interesting theoretical question whether we can have unconscious mental states as well. But it doesn't fit into the calendar that way, so I talk about these issues as part of the transition to the lectures on psychopathology and psychotherapy.
You should know how automatic processes are defined, and why they are commonly considered to be unconscious.
You should understand the distinction between explicit and implicit expressions of memory, and why implicit memory, such as priming effects, is considered to be unconscious memory.
You should also understand how the explicit-implicit distinction has been extended to perception, learning, thinking -- and, at least in principle, to emotional and motivational as well as cognitive states.
Chapter 10
Kalat devotes an entire chapter to
aspects of consciousness -- as opposed to unconscious mental
life, which was the subject of the lecture.
You should understand the notion of brain death, and the differences between coma, the vegetative state, and the minimally conscious state -- and, especially, how we can distinguish the minimally conscious state from the others.
You should know that visual stimuli can be rendered unconscious by brain damage, and in the phenomena of spatial neglect, and also by experimental manipulations, as in the case of masking and binocular rivalry.
Kalat spends a fair amount of time on the "Libet" experiment, which claimed to show that actions are initiated unconsciously, with conscious intent as a sort of afterthought. The Libet experiment was very provocative, and you should know what it was all about; but we now understand that Libet's findings were an artifact of a feature of his experimental method, and doesn't, in fact, undercut the role of conscious intent. But you wouldn't know why unless you took my course in consciousness, so you're not responsible for any criticism of the Libet experiment -- you only need to know what he did, what he found, and what he thought it meant.
You should understand the biological nature of sleep, controlled as it is by a circadian rhythm of waking and sleeping, what it means to be a "morning" or "evening" person, and the effects of shifting sleep schedules. You should know that circadian rhythms are controlled by the suprachiasmatic nucleus, which in turn regulates the release of melatonin by the pineal gland. You should know how the various stages of sleep, especially REM and NEM, are defined in terms of EEG and other physiological criteria.
You should be familiar with the basic sleep disorders: insomnia, sleep apnea, restless leg syndrome, and narcolepsy. Also the phenomena of sleepwalking, sleep talking, sleep paralysis, lucid dreams, night terrors.
You should know something about the contents of typical dreams, and especially about dreaming in blind people.
Freud's theory of dreams as wish-fulfillments is essentially invalid, but Freud is part of our cultural patrimony, so you should understand his distinction between manifest and latent contents. More important is the "activation-synthesis" theory, and Domhoff's theory of dreams as a special form of thinking, which are the best ideas we have to date.
Hypnosis is a good example of an altered state of consciousness, involving response to suggestions. You should be familiar with the use of hypnosis in the control of pain, but you should also understand some of the limitations of hypnosis -- especially with regard to the use of hypnosis to enhance memory for forgotten events, and to coerce anti-social or self-injurious behavior.
There are other altered states of
consciousness, such as meditation, and you should know about
"mindfulness" meditation and some of its effects..
Psychopathology and Psychotherapy
Finally we turned to abnormalities of mind and behavior, and what we can do about them.
You should understand what a complicated thing it is to characterize both "normal" mental functioning and "deviations" from normality: the features associated with each constitute a kind of prototype of each category. In particular, you should understand the various criteria for deviance, and the problems associated with each of them.
Historically, there have been three approaches to mental
illness: the supernatural model, which is that psychopathology
is caused by demon possession; the moral model, which is that
psychopathology is willfully assumed by the individual; and
the medical model, which is that psychopathology is the result
of natural causes that can be discovered through scientific
research. Many writers follow conventional thinking in
identifying the medical model with the idea of biological
causation, and thus biological treatment. But this is wrong:
the medical model focuses simply on natural causes, whether
biological (somatogenic) or psychosocial (psychogenic) in
nature. Still, you should understand that, at its heart, the
analogy to medical illness pervades how we talk about mental
illness:
- the distinction between signs and symptoms, syndromes, and diseases;
- talk of mental patients, mental hospitals, and mental hygiene;
- the emphasis on diagnosis;
- and, more recently, the movement toward evidence-based practices.
That's what the medical model is -- not a somatogenic theory of mental illness, or an emphasis on biological treatment (like drugs), but rather a way of thinking about mental illness: as analogous to medical illness.
In the medical model, the first step is diagnosis: classifying the illness presented by the patient. In mental illness, this is usually based on symptoms: syndromes such as schizophrenia are defined by clusters of co-occurring symptoms. The diagnostic categories are just that: categories. Traditionally, the diagnostic categories were defined in terms of features, i.e., signs and symptoms, that were singly necessary and jointly sufficient to identify a patient's illness as belonging to one category or another. But psychiatric diagnosis encountered the same sorts of problems, discussed earlier, that beset proper-set views of categorization in general. The most recent version of the Diagnostic and Statistical Manual has expressly embraced a "fuzzy set" view of categorization, emphasizing signs and symptoms that are only imperfectly correlated with category membership; and the textbook definitions of the various diagnoses serving as category prototypes. Someday, someday, the DSM will follow the example of the rest of scientific medicine and abandon diagnosis in terms of signs and symptoms for diagnosis in terms of underlying pathology (psychological or biological). But we're not there yet.
Kalat's Chapter 15 goes into some detail on the various syndromes of mental illness. You should know something about each of these major categories -- how schizophrenia is distinguished from mood disorder, for example, and how phobias and panic disorders are distinguished from generalized anxiety disorder. And you should know something about the major theories of these disorders, such as the dopamine hypothesis of schizophrenia and the serotonin hypothesis of depression.
Currently, the diagnosis of mental illness is based on signs and symptoms presented by the patient. But if we're really going to be serious about applying the medical model to psychopathology, we have to go behind (beneath?) superficial signs and symptoms to the pathological structures and processes that underlie (and cause) them. This is the task of experimental psychopathology, which includes studies of the psychological deficits characteristic of various syndromes, and also the attempt to develop laboratory models of various mental illnesses (or, at least, salient aspects of them). You should understand how laboratory paradigms have been employed to study attentional and emotional deficits in schizophrenia; how classical fear conditioning and instrumental avoidance learning have served as analogs of phobias and obsessive-compulsive disorders; and how studies of psychological deficit and laboratory models have combined to help us understand psychopathy.
Once a mental illness has been identified, the next question is where it comes from. Here, there are two opposing views, somatogenic vs. psychogenic (or organic vs. functional), roughly corresponding to nature and nurture. You should understand the relations between somatogenic and psychogenic theories of mental illness, and how a psychogenic theory can be replaced by a somatogenic theory. But even more important you should understand the diathesis-stress model of psychopathology, as reflecting the interaction of nature and nurture -- which was the subject of a whole lecture. And you should understand how behavior-genetic studies of mental illness reveal both a biological diathesis (the contribution of genes to variability) and an environmental stressor (the contribution of the nonshared environment). Remember, though, that the diathesis-stress model doesn't map precisely onto nature and nurture: the diathesis factor is often biological, but can be psychosocial; and while the stress factor is often environmental, and thus psychosocial, it can be biological.
Presumably, once we have identified the causes of mental illness, we are in a better position to treat it scientifically. In the medical model, a true cure does more than relieve symptoms: it also eliminates the underlying pathology. In terms of the diathesis-stress model, an intervention would be directed at the diathesis, the stressor, or both. In these terms, we're a long way from having a cure for most mental illnesses, but we've come a long way. You should be familiar with the popular drug treatments for the major mental illnesses, and how they relate to theories of underlying pathology. And you should be familiar with the major forms of psychotherapy, and especially psychotherapies of a cognitive-behavioral sort.
We've got a diagnostic system; we've got some theories of mental illness; we've got some treatments. The next question is: do these treatments work? This is a question that arises out of the movement toward "evidence-based healthcare", where the onus is put on health-care providers to demonstrate that treatments are effective (and cost-effective). The efficacy of drug treatments (like SSRIs for major depressive disorder) is established by clinical trials in which the effects of a new drug are compared to no-treatment controls, a placebo, or an established drug that is the current standard of care. Recently, there has been a movement to do the same sort of research on psychotherapy.
And, in fact, psychotherapy does work. The pioneering analysis by Smith, Glass, and Miller showed that the average patient who received psychotherapy did better than about 80% of patients in the control group. Initial analyses supported the "Dodo Bird Verdict" that all forms of psychotherapy were about equally effective, but closer inspection shows that, in terms of effect size, cognitive-behavioral therapies typically perform better than psychodynamic or humanistic therapies. Of particular interest is the combination of psychotherapy with drugs, and you should have some idea why combined treatment might be better than treatment with drugs or therapy alone. Sometimes, though, a complete cure is out of reach, and the patient must be helped to make the best adjustment possible to a chronic mental illness.
Traditionally, treatment (whether drugs or psychotherapy) is directed at the individual patient, but it is becoming clearer that the most effective treatments must pay attention to the individual patient's social environment. This is especially the case with family and marriage therapy. Sometimes, the individual's problems are really located in his or her family relationships; if so, the patient can't get better unless the whole family gets better as well. And it is also clear that marital problems can't be treated if just one spouse is treated: the problem is with the marriage, and so both individuals need to do some work.
There are also issues beyond the family. For example, family members make their own adjustments to an individual's mental illness, and when s/he gets better, they are going to have to change to accommodate the patient's improvement. There's a lot of stereotyping of mental illness -- for example, that the mentally ill are especially dangerous to themselves or others. And there's a lot of stigma attached to mental illness -- for example, that the mentally ill really never get better. These beliefs about mental illness affect how others will treat a mental patient -- not just while s/he is acutely ill, but also during treatment and after recovery. And, through a process known as the self-fulfilling prophecy, these beliefs can be absorbed by patients themselves -- leading them to be reluctant to seek, and comply with, treatment.
At another level, there is an
unfortunate tendency to label deviant behavior of all sorts as
a reflection of mental illness -- a trend dramatically
illustrated by the practice, in the former Soviet Union, of
isolating political dissidents in mental hospitals. And even
in our society there is a tendency to apply the moral model as
opposed to the medical model to mental illness -- to think of
the "mad" as somehow "bad".
This is part of the stigma of mental illness.
- You should know something about the nature of stigma
- Including its dimensions and components.
- How stigma can create a self-fulfilling prophecy through expectancy confirmation effects.
And you should know something about current debates about mental-health policy:
- The socio-economic burden of mental illness.
- The movement for evidence-based practices, supported by controlled clinical trials
- How this empirical support could be strengthened.
- The importance of empirically supported practices
(assessment and treatment) to the status of clinical
psychology as a profession.
Chapter 15
Kalat's Chapter 15 largely parallels
the lectures. You should know how abnormal behavior is
"officially" defined by the American Psychiatric Association,
and how the modern biopsychosocial view of abnormality differs
from traditional views (e.g., in premodern Europe, ancient
Greece, or ancient China), and how the definition of
abnormality differs from culture to culture.
You should know what the DSM is, and how it classified various mental disorders. Don't memorize the specific categories of mental illness listed in Tables 15.1 and 15.2, though you should recognize the various terms. Instead, you should know how DSM specifies the criteria for making a diagnosis -- in terms of characteristic symptoms, rather than brain damage or some other biological criterion. You should also know the weaknesses and criticisms of DSM.
You should be able to distinguish among the various anxiety disorders, and their common treatments -- which are mostly behavioral, as opposed to pharmaceutical.
You should understand the various forms of substance-abuse disorders, including the physiological processes involved in addiction, and the difference between physical and psychological dependence. Similarly, you should understand the difference between late-onset and early-onset alcoholism, and the differential role that genes and environment play in them. You should be familiar with the various treatment options available, including psycho-social and pharmaceutical options.
You should understand the various forms of mood disorder, the differential role of genes and environment (a running theme in the study of mental illness!) in depression, and how antidepressant medications work at the synaptic level. You should understand how a pessimistic explanatory style may render a person vulnerable to depression, and how this can be treated through cognitive therapy.
You should be familiar with the primary symptoms of schizophrenia, the role of genetic factors in its origin (again!), and the effects and side-effects of antipsychotic medications.
You should know the main symptoms of autism -- and that, while they are almost certainly caused by some form of brain damage, that brain damage has been extremely difficult to identify.
You should be able to distinguish
between various forms of psychotherapy, including forms of
therapy, such as family systems therapy and group therapy,
that go beyond treating the individual patient. You
should know something about the controversy over the
effectiveness of psychotherapy, and the difference between the
effects of therapy and those of a therapist.
Finally, you should know something about the social and political issues surrounding mental illness, such as involuntary commitment, the therapist's duty to protect, and the insanity defense.
Conclusion
The concluding lecture brought together many of the themes in
the course.
- Mind as the basis for intelligent action.
- We can only understand a person's behavior if we understand how he/she construed the situation.
- Cognition as an active process.
- Cognition, emotion, and motivation interact with each other.
- People actively create the situations to which they respond.
- The child is an active agent of its own development.
- Mental illness emerges from the interaction of diathesis and stress.
- Accordingly, we have to view mind in the context of biology, including evolution.
- At the same time, the legacy of biological evolution is intelligence, consciousness, and language, which together create culture.
Mind is the basis of human freedom, because it allows us to transcend the past, transform the present, and create the future.
The Cumulative Portion of the Exam
So, that's pretty much it for the
review, at least as far as the noncumulative portion of the
exam goes. For the cumulative portion, I refer you to the
reviews for Midterm 1 and Midterm 2!
This page last updated 05/15/2017.