Interview with Dr. Julianna Deardorff, Part II
In your study on condom negotiation strategies, you found that simply informing one’s partner of the risks and direct communication strategies were effective in getting the partner to use a condom, even if they initially didn’t want to. What did you learn from that study, and why aren’t condoms being used more, if something as easy as direct communication is effective?
We’re following up on that now to look at how sexual values influence condom negotiation strategies. It’s a really complicated picture, because there are different gender findings. I’m trying to go upstream right now, and look at sexual values and how they might influence the way people—the way youth, in their relationships—negotiate. And what we’re finding right now is that (this information has not been published yet) women who have more traditional sexual values tend to endorse condom negotiation strategies that focus more around using risk information to obtain condom use. So when I say “risk information,” I mean things like telling your partner you don’t want to get pregnant, that you have to be careful with STIs, and those kinds of things. And it’s very interesting because a lot of what we teach in sexual ed programs is around using direct communication and learning direct communication skills—and that is probably very good—but if it runs counter to some of your sexual values, it makes it hard to engage in that. So we’re finding that women who have less traditional values around norms and beliefs, they’re more able to use those direct communication strategies to obtain condom use from their partner. By direct communication, I mean verbal and non-verbal, so handing your partner a condom is direct as well, even though it’s not verbal.
So is that just because it’s so demanding, maybe? That’s why more “traditional” women wouldn’t want to put it that way?
Yeah, well, some of it’s not so demanding—you can do it in a non-demanding way—but I think that we have some evidence that there are strong cultural values that are endorsed around sexual talks being disrespectful within a relationship. And if you’ve been raised very traditionally, you might not feel comfortable in talking about sex in the same way as you’ve been taught in sexual health programs—it might run counter to what’s comfortable for you and what you’ve been taught. Some of the work shows that depending on some of the deep-seated cultural beliefs, there may be harder/easier strategies to use, and we should be aware of that when we’re trying to teach strategies—even when you want to use condoms, you may not be able to use certain strategies, whereas others might be more comfortable.
A lot of the sex ed that people get is in elementary school. At what age do you see people actually receiving this information?
In the work that I conduct, we see girls seeking out contraceptives. Up until last year I worked at New Generations Health Center, which is a reproductive health center in the Mission. I do counseling with youth there, and the majority of the girls there are already sexually active, and they’re past the sexual education that you’re referring to. To answer your question, youth are getting sex education in elementary school, which is great. What’s harder is that a lot of individuals are still getting the information really late—not until high school, until after they’re already having sex. I think what we really need to focus on is starting on healthy sexual development at very early ages, and that does not necessarily mean talking about sexual intercourse. Our culture doesn’t do a very good job talking about healthy sexual development, which starts at birth. If I was going to promote anything, I would promote that within families, so parents would be comfortable having conversations around positive sexual development early on. And then you wouldn’t have to have “the talk” later in life.
How would you get people to start the conversation early?
A lot of public health individuals think it needs to happen in the schools, because that is the one universal place where you have a universal audience, and I think that’s why comprehensive sexual education has become such a school-based effort. I think ideally, we could get parents on-board—I think they’re hungry for training to learn how to talk about these issues. I think there’s also a lot of variability in terms of when they want to start. I still think there’s a lot of openness among parents. I don’t think we’ve done a very good job looping parents into the process.
Do programs exist for parents to go and train themselves on how to communicate with their children about these things?
That’s a good question. I’m sure they do at local levels—probably not in a large public capacity, but I’m sure they’ve popped up. I have one colleague at UC Santa Barbara who’s developing a program for Latino moms and daughters to communicate about sex, and she has done probably some of the most culturally relevant and strong work in this area. I don’t know if anything like that is widespread, but I know there are folks in the works trying to think through these things—myself included. I’m hoping that the research I’m doing right now isn’t just going to stay just at the University, but one day, it will inform the packages of new sexual interventions and will help mothers and daughters have some of these conversations. And fathers and sons.
What about individuals that are LGBTQQI?
That’s a really good question. When we talk about healthy development, I think that we have to make sure we’re including those conversations within it.
How does that tie in with Latino youth?
It can get really complicated, because you’re overlaying some pretty strong cultural values too that have to do with same-gender relationships. What we try to do in our clinic (a sexual reproductive health clinic) is make sure we’re not assuming gender at any point in time when we’re talking to youth about their sexual relations—that we’re not putting our own assumptions onto them. Everything from the way a provider asks a question to the way he or she responds when somebody tells you about their sexual activities needs to be more inclusive, as opposed to exclusive. So at the very minimum, I think that’s where we need to start. And then when you talk about people who are transgender, marking a box on a form (whether you’re male of female) or wondering which bathroom to use at a clinic, all of that stuff really could be—and is being—revamped like in places such as San Francisco but needs to be revamped nationally so we can change our biases about these things. How does a parent talk to a child and allow that stuff to be open as well—those are the things we should be talking about in programs like school-based programs. In a sense, we’re blessed—we live in an area where there are counselors and places for people to reach out and go to.
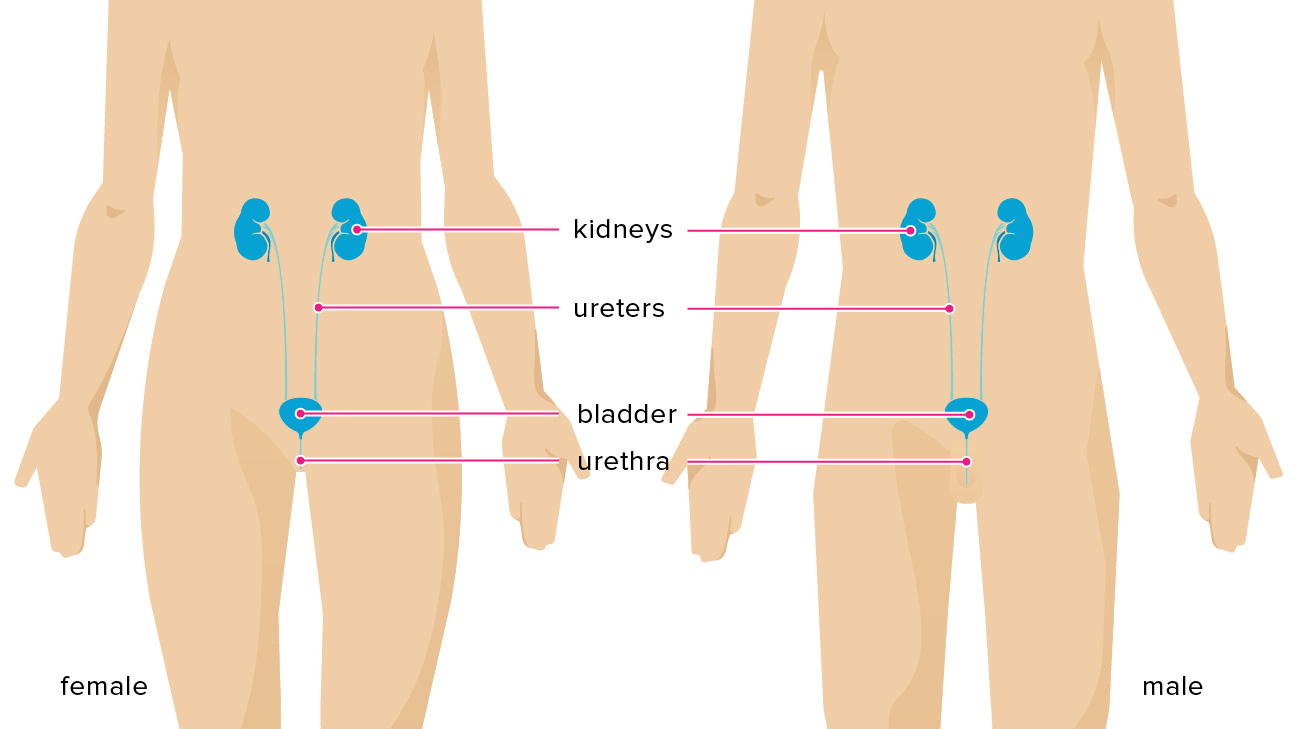
I noticed one of the risk factors that this was affecting was HIV/AIDS and how that was spread. Where is that right now in the youth in your studies?
I don’t study the prevalence of that. My work focuses on condom use behavior—which are protective. In the research work I do, we don’t know if individuals are HIV positive or not. In the clinical work I do, we of course know levels of chlamydia, gonorrhea, HPV, and other STIs, and HIV-positive individuals are really rare in our clinic. I think the important take-home message—one of the really important messages—is that condom use declines at the age range that I tend to study, which is young-adulthood. Between 18 and 24, we really see a drop in condom-use, especially in adults aged 20 to 24, and that transition between adolescence to adulthood is really key. I think that it’s interesting that they’re using condoms less, because they’re also having more sex generally. A lot of folks are getting into what they consider “monogamous” or “committed” relationships so they may stop using condoms. Whether that’s the smartest choice or not is debatable, because oftentimes when you think there’s fidelity in a relationship, there’s not. So there’s a lot of increase in STIs happening during those ages.
Do you think it’s because more females are on the pill?
I think that it may be due in part to hormonal contraceptives. I think it’s also because more people are having sex, and there tend to be more sexual partners than there were in adolescence, and like I said, I think there are also perceptions of commitment and fidelity when that’s not necessarily the case.
I think that’s really interesting, and an unseen risk factor.
Right, and I think that’s where we get into couple dynamics, like “if I ask him to wear a condom, will he think I suspect him of stepping out on me?” or “will he think I’m stepping out on him?”. These are very complicated questions, and sometimes it’s just easier not to use the condom in that moment than to have those tough conversations, despite the kind of peril you’re putting yourself in sexually.
How early do people start having sex?
You know, I think the average, except in certain pockets, is still around 15. We recently published a study on helplessness and sexual risk in sexual practices of boys and men, and the study found the number of boys having sex at or before 14 was astronomical. But, I think the average is still around 15.
Are these youth using condoms?
You know, I think that most people report using condoms at first sex, so the percentages are higher. They’re not perfect, but they’re higher. It seems that with subsequent sexual encounters, it drops off more. So it gets into relationship dynamics and how people perceive risk, and we still see in our clinics “I had sex without a condom once, and I didn’t catch anything.” That certainly still exists, even though we’ve done all we can to dispel those in these comprehensive sexual education programs.
So you’ve been talking about the clinical studies that you do and why you’re doing certain research studies. Now, could you please tell us a little more about what your career looks like? For students who are interested in psychology and related research, we would also like to know what you did to get to where you are today?
I was always interested in behavior and sexuality. And I went into clinical psychology because I wanted to understand more of the behavior factors that underlie a lot of those prevalent traits. So I started out in clinical psychology and, up until January, I was doing clinical practice at UCSF, which was before I was at Berkeley, and at an adolescent teen clinic. I felt like it made my research very real, and I miss it. So I plan on going back to doing work like that again. I’ve done a lot of community-based work, too.
Right now, because of my career, my day-to-day looks a lot like a technical assistant professor, where you’re teaching and you’re doing a little bit of service. Most of who I’ve been teaching has been graduate students because I’m in the School of Public Health. And then there’s also the research side of my work and getting papers out. It’s just over the course of your professional career where your focus is. I meet with a lot of students and a lot of colleagues, and there are just a lot of research programs going on right now. And every once in a while, I’ll do some evaluation and consulting in different parts of the world.
But I would say what I like about having a clinical degree is that it does allow me to stay in very close touch with the population I study and the issues that I’m interested in—it keeps it very alive and dynamic for me.
Article by Nikita Rathaur
Feature Image Source: MastersDegree.net